424B3: Prospectus filed pursuant to Rule 424(b)(3)
Published on April 6, 2015
Table of Contents
| Prospectus | Filed Pursuant to Rule 424(b)(3) Registration Statement No. 333-198563 |
Corbus Pharmaceuticals Holdings, Inc.

19,470,273 Shares
Common Stock
This prospectus relates to the offer for sale of up to an aggregate of 19,470,273 shares of common stock of Corbus Pharmaceuticals Holdings, Inc. by the selling stockholders named herein. We are not offering any securities pursuant to this prospectus. The shares of common stock offered by the selling stockholders include 10,636,174 shares of common stock underlying warrants with an exercise prices ranging from $0.60 to $1.00 per share.
Our common stock is quoted on the Over-the-Counter Markets, or OTC.QB, under the symbol CRBP. On April 2, 2015, the last reported sale price for our common stock on the OTC.QB was $2.90 per share.
Certain of the selling stockholders and intermediaries, who are identified as broker-dealers in the footnotes to the selling stockholder table contained in this prospectus, through whom such securities are sold are deemed underwriters within the meaning of the Securities Act of 1933, as amended, with respect to the securities offered hereby, and any profits realized or commissions received may be deemed underwriting compensation. We believe that all securities purchased by broker-dealers or affiliates of broker-dealers were purchased by such persons and entities in the ordinary course of business and at the time of purchase, such purchasers did not have any agreements or understandings, directly or indirectly, with any person to distribute such securities.
Investing in our common stock is highly speculative and involves a significant degree of risk. See Risk Factors beginning on page 10 of this prospectus for a discussion of information that should be considered before making a decision to purchase our common stock. We are an emerging growth company under the federal securities laws and, as such, we intend to comply with certain reduced public company reporting requirements.
Neither the Securities and Exchange Commission nor any state securities commission has approved or disapproved of these securities or determined if this prospectus is truthful or complete. Any representation to the contrary is a criminal offense.
The date of this prospectus is April 6, 2015.
Table of Contents
| 1 | ||||
| 9 | ||||
| 10 | ||||
| 30 | ||||
| 31 | ||||
| 31 | ||||
| 32 | ||||
| 47 | ||||
| 52 | ||||
| 60 | ||||
| 62 | ||||
| 64 | ||||
| 68 | ||||
| 75 | ||||
| 77 | ||||
| 77 | ||||
| 77 | ||||
| DISCLOSURE OF COMMISSION POSITION ON INDEMNIFICATION FOR SECURITIES ACT LIABILITIES |
78 | |||
| 78 | ||||
| 79 | ||||
| II-6 | ||||
You should rely only on the information contained in this prospectus. We have not authorized any other person to provide you with information different from or in addition to that contained in this prospectus. If anyone provides you with different or inconsistent information, you should not rely on it. We are not making an offer to sell these securities in any jurisdiction where an offer or sale is not permitted. You should assume that the information appearing in this prospectus is accurate only as of the date on the front cover of this prospectus. Our business, financial condition, results of operations and prospects may have changed since that date.
For investors outside the United States: We have not done anything that would permit this offering or possession or distribution of this prospectus in any jurisdiction where action for that purpose is required, other than in the United States. You are required to inform yourselves about and to observe any restrictions relating to this offering and the distribution of this prospectus.
In this prospectus, we rely on and refer to information and statistics regarding our industry. We obtained this statistical, market and other industry data and forecasts from publicly available information.
Table of Contents
This summary highlights information contained in other parts of this prospectus. Because it is a summary, it does not contain all of the information that you should consider in making your investment decision. Before investing in our common stock, you should read the entire prospectus carefully, including our consolidated financial statements and the related notes included in this prospectus and the information set forth under the headings Risk Factors and Managements Discussion and Analysis of Financial Condition and Results of Operations.
When used herein, unless the context requires otherwise, references to the Company, Holdings, we, our and us refer to Corbus Pharmaceuticals Holdings, Inc., a Delaware corporation, collectively with its wholly-owned subsidiary, Corbus Pharmaceuticals, Inc., a Delaware corporation.
Our Company
General
We are a clinical stage biopharmaceutical company, focused on the development and commercialization of novel therapeutics to treat rare, life-threating inflammatory-fibrotic diseases with clear unmet medical needs. Our product Resunab, or Resunab, is a novel oral anti-inflammatory drug that is expected to commence Phase-IIa clinical trials for the treatment of scleroderma and cystic fibrosis, or CF, during the second quarter of 2015.We submitted an Investigational New Drug Application or IND, to the U.S. Food and Drug Administration, or FDA, for Resunab with the scleroderma clinical protocol on February 5, 2015. On March 5, 2015, we received FDA authorization to initiate the scleroderma clinical trial. During the second quarter of 2015, we plan to submit to the FDA under the Resunab IND an additional clinical protocol for cystic fibrosis.
Corbus Pharmaceuticals, Inc. (formerly known as JB Therapeutics, Inc.), was incorporated on April 24, 2009 under the laws of the State of Delaware. On April 11, 2014, JB Therapeutics, Inc. completed a merger with Corbus Pharmaceuticals Holdings, Inc. and changed its name to Corbus Pharmaceuticals, Inc. Upon the consummation of the merger, Corbus Pharmaceuticals, Inc. became a wholly owned subsidiary of Corbus Pharmaceuticals Holdings, Inc., or Corbus, which continues to operate the business of Corbus Pharmaceuticals, Inc. Since our inception, we have devoted substantially all of our efforts to business planning, research and development, recruiting management and technical staff, acquiring operating assets and raising capital. Our research and development activities have included completing pre-clinical studies, the development of manufacturing methods and manufacturing of our lead drug Resunab for clinical trials and the design of clinical protocols for human clinical studies.
Inflammation is a natural defense mechanism carried out by our immune system to protect our bodies from infection and injury. However, under certain circumstances inflammation once triggered is unable to be resolved, resulting in a chronic inflammatory disease. Since each organ in the body is capable of protecting itself from infection and injury by recruiting inflammatory cells to its site, each organ has the potential to suffer from excessive inflammation leading to inflammatory diseases that may cause discomfort, pain, loss of organ function, disability or even death. There are hundreds of inflammatory diseases, many of which are chronic, life-long and incurable.
A key aspect of the bodys inflammatory response is the recruitment of inflammatory cells to the site of tissue infection/injury whereupon these cells act to destroy the infection and/or repair tissue damage. The signaling pathway that modulates the inflammatory response involves the production of bioactive lipids termed eicosanoids by the enzymes cyclooxygenase, or COX, and lysyl oxidase, or LOX, resulting in pro-inflammatory mediators as shown in the Figure 1 below. These mediators trigger the activation and maintenance of a cellular inflammatory state resulting in the further generation of pro-inflammatory mediators termed cytokines. This fundamental pathway is involved in a wide spectrum of inflammatory diseases.
While the onset of inflammation has been well understood for some time, the mechanisms that resolve inflammation have only recently been discovered. This resolution pathway involves shifting the production of pro-inflammatory eicosanoids by the COX and LOX enzymes to the production of anti-inflammatory eicosanoids. These anti-inflammatory eicosanoids act to resolve inflammation and promote tissue healing. The lack of sufficient inflammatory resolution is a key contributor to many chronic inflammatory diseases.
Resunab is a synthetic, rationally designed oral small molecule that selectively binds to CB2 receptors found on immune cells. The CB2 receptor plays a natural role in modulating and resolving inflammation by, in effect, turning inflammation off. Through activation of CB2, Resunab stimulates the production of anti-inflammatory mediators and causes a concomitant reduction in pro-inflammatory mediators and cytokines. Because it acts through this natural resolving pathway, Resunab offers a new mechanism to potentially treat a wide spectrum of chronic inflammatory diseases in which the resolution of inflammation (the off switch) fails to occur.
1
Table of Contents
Figure 1: the ON and OFF cellular inflammatory pathways
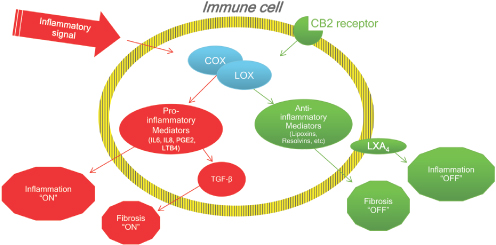
In many chronic diseases, unresolved inflammation causes progressive damage to tissues and organs resulting in excessive tissue scarring, or fibrosis, that leads to organ failure and death. Examples of such chronic diseases include cystic fibrosis, scleroderma, liver cirrhosis and non-alcoholic steatohepatitis, or NASH, chronic kidney disease, muscular dystrophies, rheumatoid arthritis systemic lupus erythematosus and myositis. Resunab has demonstrated pre-clinical efficacy in a number of inflammatory and fibrotic disease animal models. In inflammatory models it was shown to reduce the migration of inflammatory cells into the site of inflammation, stimulate the production of the resolving (anti-inflammatory) eicosanoids, and down-regulate and reduce pro-inflammatory mediators and cytokines. In fibrosis models it was shown to reduce tissue collagen production, tissue fibrosis, stimulate the production of the resolving (anti-inflammatory) eicosanoids and reduce the pro-fibrotic cytokine TGF-beta. The net result is that Resunabthrough activation of CB2triggers a natural inflammatory resolution pathway and is therefore expected to offer a new and promising mechanism for the potential treatment of chronic inflammation and fibrosis.
Our Pipeline
The development status of Resunab is summarized below:
Figure 2: Drug developmental pipeline
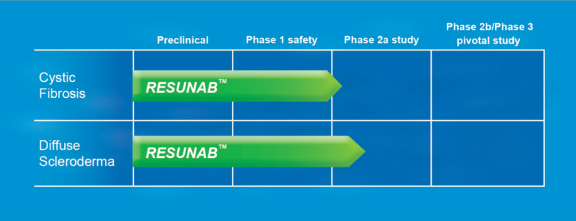
Pre-clinical studies and Phase-I human safety studies (n=136) for Resunab have been completed that support our Phase II clinical development plan. Prior Phase 1 safety studies were conducted by Atlantic Pharmaceuticals, Inc. in 2001-2002 and by Cervelo Pharmaceuticals as sub licensee to Indevus Pharmaceuticals in 2008. We expect to rely on this data from these studies in addition to the pre-clinical data generated by us to file our INDs and launch directly into Phase 2 clinical studies for scleroderma and cystic fibrosis. We previously submitted a summary of the prior preclinical and clinical data and held a preIND meeting with the FDA division of Pulmonology, Allergy and
2
Table of Contents
Rheumatology on October 26, 2012 to discuss the prior preclinical and Phase 1 data and to discuss our planned clinical development program for Systemic Sclerosis. The FDA advised us, that prior to filing an IND, we needed to conduct a rat chronic toxicology study and obtain an acceptable safety margin of >1X, the no-observed effect level. We completed this chronic rat toxicology study and successfully achieved the necessary safety margin. Human clinical studies to-date show Resunab has good oral bioavailability, is well tolerated and causes no serious adverse effects at therapeutic levels. Resunab exhibited none of the serious adverse side effects that are associated with routinely used anti-inflammatory drugs: the gastrointestinal side effects of non-steroidal anti-inflammatory drugs, or NSAIDs, and the metabolic side effects of corticosteroids. The safety data to-date suggests that Resunab has an acceptable therapeutic dosing window and is well tolerated, making the treatment of chronic inflammatory and fibrotic diseases attractive therapeutic indications for the drug. We received clearance from the FDA for the IND for scleroderma in March 2015 and expect to commence Phase IIa clinical studies for cystic fibrosis and scleroderma during the second quarter of 2015.
Cystic Fibrosis
Cystic fibrosis, or CF, is an incurable disease caused by a mutation in the gene Cystic Fibrosis Transmembrane Conductance Regulator, or CFTR, that results in aberrant chloride ion transport leading to the accumulation of thick, viscous secretions in certain tissues, including the lung, pancreas and gastrointestinal tract. The most common symptom in CF is pulmonary dysfunction. The genetic defect in CF triggers chronic inflammation causing both morbidity and, ultimately, mortality. CF patients lungs are exposed to a vicious cycle of obstruction, infection and inflammation, which are all intimately linked and gradually lead to pulmonary fibrosis and deterioration in breathing capacity, eventually resulting in death. The current life expectancy of CF patients averages 40 years. According to the Cystic Fibrosis Foundation, 30,000 Americans and a total of 70,000 people worldwide suffer from CF. Current therapies for CF include antibiotics to fight bacterial infection, mucolytics to digest mucus buildup and, very recently, correctors which act to repair faulty CFTR activity in specific genetic sub-populations of patients (Kalydeco). The cost of treating CF is very high, with an average cost in the U.S. of $49,000 per patient per annum (based on research published in 2011). The recent addition of Kalydeco, approved in January 2012, has an annual cost of $307,000 per patient but can reach up to $370,000 for certain patients. However, with at least 1,300 different known mutations in the CFTR gene, Kalydeco can only be used by a specific sub-section of the CF population who suffer from a limited number of gating mutations, including the G551D mutation. Combined, these currently account for about 4.5% of the total CF patient population in the United States.
During the second quarter of 2015, we plan to submit an additional clinical protocol under the Resunab IND for a Phase IIa double-blind placebo controlled study evaluating Resunab in CF at initial dosing levels for the first month of 1mg and 5mg per day and then 20 mg once a day and 20 mg twice a day, versus placebo. We expect to initiate the clinical study during the second quarter of 2015. Patients in the study will be 18-30 years of age with mild to moderate cystic fibrosis as assessed by lung function tests. The trial design will have a two-week screening period, followed by a 12-week active treatment period, and then a four-week safety follow-up. The study planned is a multi-center U.S. and European trial. The lead Principal Investigators in the U.S. will be Dr. James Chmiel of the Rainbow Babies & Childrens Hospital, Cleveland, Ohio and in the E.U., Dr. Stuart Elborn of Queens University Hospital, Belfast, Ireland. Patients will be screened and those meeting the trial criteria will be randomized into one of four arms. Patients will be monitored for safety and tolerability throughout the study. The primary goal of this trial is to establish safety of Resunab in CF patients and an efficacy assessment based on pulmonary function and the reduction of inflammatory markers. Secondary efficacy assessments will include the CF biomarker score, patient scores and drug action biomarkers.
Scleroderma
Scleroderma is a chronic connective tissue disease characterized by the thickening of the skin and is generally classified as an autoimmune rheumatic disease. According to the Scleroderma Foundation, about 300,000 Americans have scleroderma with one third having the systemic form. The disease affects mainly adults (80% of scleroderma patients are women) with onset typically in the patients 30s or 40s. Systemic scleroderma can affect multiple organs in the body. The tissues of affected organs become hard and fibrous, adversely affecting their function. There are two major recognized sub-categories of systemic scleroderma diffuse and limited with each representing about 50% of systemic scleroderma patients. Approximately 50,000 Americans have diffuse scleroderma, which indicates increased risk for fibrosis of the internal organs. Diffuse scleroderma patients have a high mortality rate with approximately 50% survival over a 10 year period. There are currently no cures or effective therapies for diffuse scleroderma.
On February 5, 2015, we submitted an IND to the FDA for Resunab with the clinical protocol for a Phase IIa double-blind placebo controlled clinical study evaluating Resunab in patients with diffuse scleroderma at three dosing levels, 5 mg and 20 mg once-a-day and 20 mg twice a day, versus placebo. On March 5, 2015, we received FDA authorization to initiate the scleroderma clinical trial and we expect to initiate the trial during the second quarter of 2015. The trial design will have a four-week screening period, 12-week treatment period and a four-week safety follow-up. The study planned is a U.S. multi-center trial. The lead Principal Investigator will be Dr. Robert Spiera of the Hospital of Special Surgery, New York City, New York. Patients will be screened and those meeting trial criteria will be randomized to one of four arms. Patients will be monitored for safety and tolerability throughout the study. The primary goal of this trial is to establish safety of Resunab in diffuse scleroderma patients and efficacy based on a change in the Combined Response Index in diffuse cutaneous Systemic Sclerosis. Secondary endpoint measurements will include patient assessment scores, drug action biomarkers, disease biomarkers and metabolipidomic profiles.
3
Table of Contents
Our Strategy
Our business strategy is to develop and commercialize novel proprietary inflammatory-resolution pharmaceuticals for the treatment of serious life-threatening chronic inflammatory diseases for which there are no safe and effective treatments. Resunab has a unique mechanism of action with the potential to treat inflammation and fibrosis in a broad number of chronic inflammatory diseases. Promising opportunities exist to expand our markets beyond cystic fibrosis and scleroderma with additional indications for Resunab including fibrotic liver diseases (such as NASH), chronic kidney disease, muscular dystrophy, dermatomyositis and lupus. We believe Resunab has the potential to serve an unmet medical need in treating serious chronic inflammatory diseases by offering a potent medicine which can be given chronically to treat chronic inflammation and fibrosis with minimal adverse side effects. In addition to Resunab, we will endeavor to expand our pipeline by licensing in other novel drug candidates which target high unmet medical conditions through the resolution of inflammation and fibrosis.
Our objective is to enter into strategic license arrangements with pharmaceutical companies for the commercialization of our drug products. This process will involve completing pivotal clinical trials and obtaining regulatory approvals for the manufacturing, marketing, distribution and sale of our drugs. We have an experienced management team to implement our business strategy with many years of expertise in drug development.
Formation of Holdings
We are a Delaware corporation. In connection with our formation in December 2013, we sold an aggregate of 6,000,000 shares of common stock for an aggregate of $120,000 ($0.02 per share), which includes 1,000,000 shares of common stock owned by Adam Stern. Mr. Stern is an affiliate of Aegis Capital Corporation, or Aegis Capital, the placement agent in our 2014 private placement described below.
Recent Developments
The Merger Transaction
On March 27, 2014, JB Therapeutics, Inc., or JB Therapeutics, entered into a merger agreement by and among JB Therapeutics, Holdings, and Corbus Pharmaceuticals Acquisition, Inc. a Delaware corporation and our wholly-owned subsidiary, or Merger Sub. Pursuant to the terms of the merger agreement, as a condition of and contemporaneously with the initial closing of the 2014 Private Placement, or the Initial Closing, described below, Merger Sub merged with and into JB Therapeutics and JB Therapeutics became a wholly-owned subsidiary of us. In connection with the merger, or the Merger, stockholders of JB Therapeutics received an aggregate of 9,000,000 shares of our common stock and the preferred stockholders of JB Therapeutics also received warrants, or the Merger Warrants, to purchase 917,612 shares of our common stock at an initial exercise price of $1.00 per share. In addition, the holders of warrants to purchase common stock of JB Therapeutics prior to the Merger received warrants, or the Replacement Warrants, to purchase 27,839 shares of our common stock with an exercise price of $0.60. Except for the exercise price, the terms of the Merger Warrants and the Replacement Warrants are substantially similar to the Investor Warrants. We also issued warrants, or the Additional Replacement Warrants, to purchase 350,000 shares of our common stock, with an exercise price of $0.66, to replace previously held warrants to purchase common stock of JB Therapeutics. The Additional Replacement Warrants are substantially similar to the Investor Warrants except that they include cashless exercise provisions and are not subject to redemption by us. In connection with the Merger, holders of outstanding options of JB Therapeutics received, in substitution for such options, options to purchase an aggregate of 905,334 shares of our common stock with exercise prices ranging from $0.11 to $0.17 per share. At the closing of the merger, the board of directors of Holdings consisted of Yuval Cohen, the Chief Executive of Corbus and former Chief Executive Officer of JB Therapeutics, Alan Holmer a former Director of JB Therapeutics, and David Hochman, a Board designee of Aegis Capital.
The Merger was treated as a reverse acquisition and recapitalization of JB Therapeutics for financial accounting purposes and the historical financial statements of JB Therapeutics are our financial statements as a result of the Merger. The parties to the Merger Agreement have agreed to take all actions necessary to ensure the Merger is treated as a plan of reorganization under Section 368(a) of the Internal Revenue Code of 1986, as amended.
2014 Private Placement
We conducted a private placement offering in April and May 2014 with four closings with the final closing occurring on May 30, 2014. We issued an aggregate 10,260,000 shares of our common stock and warrants, or the Investor Warrants, to purchase 10,260,000 shares of our common stock at an exercise price of $1.00. The Investor Warrants are exercisable for a period of five years from the date of grant. Gross proceeds totaled $10,260,000 and net proceeds were $8,402,000. Aegis Capital Corp. acted as the Placement Agent, or the Placement Agent, for the 2014 Private Placement. Pursuant to the registration statement of which this prospectus is a part, we are registering the shares of common stock and shares of common stock underlying the Investor Warrants issued in the 2014 Private Placement for public resale by the selling stockholders named herein and their assigns.
4
Table of Contents
In connection with the 2014 Private Placement, we paid the Placement Agent and selected dealers an aggregate cash fee of $1,023,000, we paid the Placement Agent a non-accountable expense allowance equal to $308,000, and we incurred $527,000 of other expenses related to the financing. In addition, as part of its compensation for acting as placement agent for the 2014 Private Placement, we issued a warrant, or the Placement Agent Warrants, to the Placement Agent to purchase 2,047,000 shares of our common stock with an exercise price of $1.00 per share. Such warrants contain a cashless exercise feature and are exercisable at any time prior to five years from the date of grant.
Our Risks
An investment in our common stock involves a high degree of risk. You should carefully consider the risks summarized below. These risks are discussed more fully in the Risk Factors section of this prospectus immediately following this prospectus summary. These risks include, but are not limited to, the following:
| | we have a limited operating history and have incurred operating losses of approximately $4.4 million from inception through December 31, 2014 and we expect to incur substantial losses for the foreseeable future and may never achieve or maintain profitability which could materially limit our ability to raise additional funds through the issuance of new debt or equity securities or otherwise; |
| | we will need to obtain additional financing to complete clinical development of Resunab; |
| | clinical trials for our product candidate, Resunab, may not be successful and we may not obtain approval from the FDA or other regulatory bodies in different jurisdictions for Resunab; |
| | we are highly dependent on the success of our product candidate, Resunab, which is still in early stage development; |
| | we expect to rely on third parties to manufacture Resunab and to conduct our clinical trials; |
| | we currently do not have the infrastructure to commercialize Resunab should we be successful in obtaining FDA approval; |
| | we face significant competition from other biotechnology and pharmaceutical companies; |
| | even if we obtain marketing approval for Resunab, we will be subject to ongoing obligations and continued regulatory review; and |
| | we rely on our key employees and executives and the loss of the services of our key employees and executives would adversely impact our business prospects. |
Reverse Stock Split Range Authorization
Our board of directors and stockholders have approved a reverse stock split (the Reverse Stock Split Amendment Authorization) within a range of 1:1.25 to 1:5 (the reverse stock split range). The Reverse Split Amendment Authorization permits us to maintain flexibility to effect a reverse stock split if our board of directors should determine that a reverse stock split is in the best interest of our stockholders and us. While our board of directors has not determined to effect a reverse stock split, it may determine that effecting a reverse stock split is necessary in connection with our ability to satisfy the initial listing requirements to support our application to be listed on NASDAQ Stock Market (NASDAQ) or NYSE MKT.
We will file a reverse stock split amendment to the Certificate of Incorporation only in the event that our board of directors deems it advisable, such as, for example, in connection with our future listing on an exchange or for the purpose of enhancing investor interest generally. Should the reverse stock split be effected, upon the effectiveness of the amendment to our Certificate of Incorporation, (the Split Effective Time), the issued shares of our common stock immediately prior to the Split Effective Time will be reclassified into a smaller number of shares such that a stockholder will own one new share of our common stock for each of either 1.25 to 5 shares of issued shares of our common stock held by that stockholder immediately prior to the Split Effective Time. If our board of directors deems a reverse stock split to be advisable, the exact reverse stock split ratio within the reverse stock split range will be determined by our board of directors prior to the Split Effective Time and will be publicly announced by us. The par value of each share of our common stock shall be maintained at $0.0001 per share for the reduced number of shares after any such reverse stock split. Even if our stockholders approve the reverse stock split, we may only effect the reverse stock split if such reverse stock split is effected on or before the date that is the earlier of one year from the date we receive stockholder approval and the date our next annual meeting of stockholders is held.
5
Table of Contents
Purpose
If we effect the reverse stock split, it will be based upon the following considerations:
| | Future Listing Applications. We may in the future apply for listing on a national securities exchange such as NASDAQ or NYSE MKT which includes in its initial listing standards a minimum price per share that could be greater than the then current price per share of our common stock. |
| | Enhanced Investor Interest. A higher stock price resulting from a reverse stock split could help generate investor interest and allow a wider range of investors to purchase our common stock, help facilitate future financings or increase our ability to use our capital stock in acquisitions, although there can be no assurance that a reverse stock split would result in any of the foregoing. |
Requirements for Listing on Other Exchanges or Markets
We may also consider an application for listing of our common stock on NASDAQ or NYSE MKT or other markets in or outside of the United States. Any such listing may require the market price of our common stock to be increased above its then current level. While authorization to effect a reverse stock split may be helpful in achieving any such relevant minimum share price, a reverse stock split would not guarantee that our common stock would achieve any such relevant minimum price.
Potential Increased Investor Interest
A low share price can reduce the effective marketability of stocks because of the reluctance of some brokerage firms to recommend low-priced stocks to their clients and because many institutional investors generally do not invest in low-priced stocks. Further, a variety of brokerage house policies and practices tend to discourage individual brokers within those firms from dealing in low-priced stocks. Some of those policies and practices pertain to the payment of brokers commissions and to time-consuming procedures that function to make the handling of low-priced stocks unattractive to brokers from an economic standpoint. In addition, the structure of trading commissions also tends to have an adverse impact upon holders of low-priced stocks because the brokerage commission on a sale of low-priced stock generally represents a higher percentage of the sales price than the commission on a relatively higher-priced stock. We believe that the reverse stock split may result in a higher trading range for our common stock and may encourage institutional investors to invest in, and brokerage houses to recommend, our common stock. If the reverse stock split is effected, the market price of our common stock will also be based on our performance and other factors unrelated to the number of shares outstanding.
Principal Effects of the Reverse Stock Split
In the event we determine to effect the reverse stock split, the Certificate of Amendment would effect the reverse stock split but would not change the number of authorized shares of our common stock or preferred stock, or the par value of the our common stock or preferred stock.
In the event the reverse stock split is effected, it will be effected simultaneously for all outstanding shares of our common stock. The reverse stock split will affect all of our stockholders uniformly and will not affect any stockholders percentage ownership interests in us, except to the extent that the reverse stock split results in any of our stockholders owning a fractional share, in which case such fractional share will be paid in cash. Shares of our common stock issued pursuant to the reverse stock split will remain fully paid and nonassessable.
As shown in the table below, in the event the reverse stock split is effected, one of its effects will be to effectively increase the proportion of authorized shares which are unissued relative to those which are issued. This could result in our management being able to issue more shares without further stockholder approval. We believe that the continued availability of sufficient shares of our common stock is necessary and desirable to provide us with the flexibility of engaging in future equity financings or acquisitions utilizing our common stock.
The following table provides estimates as of March 12, 2015 of the number of shares of our common stock (a) authorized, (b) issued and outstanding, (c) reserved for issuance and (d) authorized but neither issued nor reserved for issuance at the following times: (i) prior to any reverse stock split, (ii) in the event a reverse stock split is effected and it is at a 1:1.25 ratio and (iii) in the event a reverse stock split is effected and it is at a 1:5 ratio:
6
Table of Contents
| Number of Shares of Common Stock Authorized |
Number of Shares Issued and Outstanding (1) |
Number of Shares Reserved for Future Issuance (2) |
Number of Shares Authorized but Neither Issued nor Reserved for Future Issuance (1)(2) |
|||||||||||||
| Prior to Any Reverse Stock Split |
150,000,000 | 26,003,304 | 20,409,491 | 103,587,205 | ||||||||||||
| After assumed 1:1.25 Reverse Stock Split |
150,000,000 | 23,114,048 | 18,141,770 | 108,744,182 | ||||||||||||
| After Assumed 1:5 Reverse Stock Split |
150,000,000 | 5,200,661 | 4,081,898 | 140,717,441 | ||||||||||||
(1) These estimates assume a total of 26,003,304 shares of common stock issued and outstanding immediately prior to the reverse stock split, which is based on the 26,003,304 shares issued and outstanding as of March 12, 2015.
(2) The following 20,409,491 shares of common stock are included in the Number of Shares Reserved for Future Issuance: (i) outstanding options to purchase 3,556,691 shares of our common stock with exercise prices ranging from $0.11 to $3.30 per share; (ii) up to 3,205,952 shares of our common stock that are available for issuance under our stock option plan; (ii) warrants exercisable for 10,266,667 shares of common stock at an exercise price of $1.00 per share issued in our 2014 Private Placement, (iii) warrants exercisable for 882,322 shares of our common stock at an exercise price of $1.00 per share issued in connection with the merger we completed in 2014, (iv) warrants exercisable for 27,839 shares of our common stock at an exercise price of $0.60 per share, (v) warrants exercisable for 350,000 shares of our common stock at an exercise price of $0.66 per share, (vi) warrants exercisable for 162,359 shares at an exercise price of $1.00 per share and (vii) warrants exercisable for 2,025,500 shares of our common stock at an exercise price of $1.00 per share issued to our placement agent in connection with the 2014 Private Placement. The Number of Shares Reserved for Future Issuance is based on 20,409,491 shares reserved for future issuances on March 12, 2015.
Par Value
In the event the reverse stock split is effected, the par value of our common stock will remain at $0.0001 per share, the same pre-reverse stock split as post-reverse stock split. If the reverse stock split is effected, the total stated capital will be reduced and additional paid-in capital will be increased in the same amount, as discussed below.
Potential Anti-Takeover Effect
Although the increased proportion of unissued authorized shares to issued shares could, under certain circumstances, have an anti-takeover effect, for example, by permitting issuances that would dilute the stock ownership of a person seeking to effect a change in the composition of our board of directors or contemplating a tender offer or other transaction for the combination of us with another company, the reverse stock split proposal is not being proposed in response to any effort of which we are aware to accumulate shares of our common stock or to obtain control of us, nor is it part of a plan by management to recommend a series of similar amendments to our board of directors and stockholders. Our board of directors does not currently contemplate recommending the adoption of any other actions that could be construed to affect the ability of third parties to take over or change control of us.
Odd Lots
In the event the reverse stock split is effected, it will result in an increased number of stockholders owning odd lots of fewer than 100 shares of our common stock after the reverse stock split. The per share costs, including brokerage commissions, of transactions in odd lots, are generally higher than the costs of transactions in round lots of multiples of 100 shares.
7
Table of Contents
Notification of Reverse Stock Split Effectiveness
In the event the reverse stock split is effected, as soon as practicable after the Split Effective Time, stockholders will be notified that the reverse stock split has been effected through the filing by us of a press release and a filing with the Securities and Exchange Commission. Our transfer agent will act as the exchange agent for purposes of implementing the exchange of stock certificates. Holders of pre-reverse stock split shares will be able to surrender to the exchange agent certificates representing pre-split shares in exchange for certificates representing post-reverse stock split shares in accordance with the procedures to be set forth in a letter of transmittal to be sent by us.
Implications of Being an Emerging Growth Company
We are an emerging growth company, as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act, and, for as long as we continue to be an emerging growth company, we may choose to take advantage of exemptions from various reporting requirements applicable to other public companies but not to emerging growth companies, including, but not limited to, not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act of 2002, reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements, and exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and stockholder approval of any golden parachute payments not previously approved. We could be an emerging growth company for up to five years, or until the earliest of (i) the last day of the first fiscal year in which our annual gross revenues exceed $1 billion, (ii) the date that we become a large accelerated filer as defined in Rule 12b-2 under the Securities Exchange Act of 1934, as amended, which would occur if the market value of our common stock that is held by non-affiliates exceeds $700 million as of the last business day of our most recently completed second fiscal quarter, or (iii) the date on which we have issued more than $1 billion in non-convertible debt during the preceding three-year period. We are choosing to opt out of the extended transition periods available under the JOBS Act for complying with new or revised accounting standards, and intend to take advantage of the other exemptions.
Corporate Information
We are a Delaware corporation formed in 2013 under the name SAV Acquisition Corp. In February 2014, we changed our name to Corbus Pharmaceuticals Holdings, Inc. We are the parent company of Corbus Pharmaceuticals, Inc., our operating subsidiary, a Delaware corporation, which changed its name from JB Therapeutics, Inc. following the Merger.
Our principal offices are located at 100 River Ridge Drive, Norwood, MA 02062. Our web address is www.corbuspharma.com. Information contained in or accessible through our web site is not, and should not be deemed to be, part of this prospectus.
We currently do not own or license any U.S. federal trademark registrations or applications. Some trademarks referred to in this prospectus are referred to without the ® and symbols, but such references should not be construed as any indicator that their respective owners will not assert, to the fullest extent under applicable law, their rights thereto. We do not intend the use or display of other companies trademarks and trade names to imply a relationship with, or endorsement or sponsorship of us by, any other companies.
8
Table of Contents
| Common Stock Outstanding | 26,003,304 shares (1) | |
| Common Stock Offered by Selling Stockholders | 19,470,273 shares (2) | |
| Use of Proceeds | We will not receive any proceeds from the sale of the common stock by the selling stockholders. We would, however, receive proceeds upon the exercise of the warrants held by the selling stockholders which, if such warrants are exercised in full, would be approximately $10,544,853. Proceeds, if any, received from the exercise of such warrants will be used for working capital and general corporate purposes. No assurances can be given that any of such warrants will be exercised. | |
| Quotation of Common Stock | Our common stock is quoted on the OTC.QB under the symbol CRBP. The 19,470,273 shares of our common stock can be sold by selling stockholders at prevailing market prices or privately negotiated prices on the OTC.QB. | |
| Risk Factors | An investment in our company is highly speculative and involves a significant degree of risk. See Risk Factors and other information included in this prospectus for a discussion of factors you should carefully consider before deciding to invest in shares of our common stock. | |
| (1) | Excludes: (i) outstanding options to purchase 3,556,691 shares of our common stock exercise prices ranging from $0.11 to $3.30 per share; (ii) up to 3,205,952 shares of our common stock that are available for issuance under our stock option plan; (ii) Investor Warrants exercisable for 10,266,667 shares of common stock at an exercise price of $1.00 per share issued in our 2014 Private Placement, (iii) Merger Warrants exercisable for 855,483 shares of our common stock at an exercise price of $1.00 per share issued in connection with the Merger, (iv) Replacement Warrants exercisable for 27,839 shares of our common stock at an exercise price of $0.60 per share, (v) Additional Replacement Warrants exercisable for 350,000 shares of our common stock at an exercise price of $0.66 per share, and (vi) the Placement Agent Warrants exercisable for 2,025,500 shares of our common stock at an exercise price of $1.00 per share. |
| (2) | Includes: (i) 9,441,667 shares of our common stock underlying the Investor Warrants, which have an exercise price of $1.00 per share, (ii) 855,483 shares of our common stock underlying the Merger Warrants, which have an exercise price of $1.00 per share, (iii) Replacement Warrants exercisable for 27,839 shares of common stock at an exercise price of $0.60 per share issued to existing warrant holders in JB Therapeutics, and (iv) Additional Replacement Warrants exercisable for 350,000 shares of common stock at an exercise price of $0.66 per share. |
9
Table of Contents
An investment in our common stock is speculative and illiquid and involves a high degree of risk including the risk of a loss of your entire investment. You should carefully consider the risks and uncertainties described below and the other information contained in this prospectus before purchasing shares of our common stock. The risks set forth below are not the only ones facing us. Additional risks and uncertainties may exist that could also adversely affect our business, operations and prospects. If any of the following risks actually materialize, our business, financial condition, prospects and/or operations could suffer. In such event, the value of our common stock could decline, and you could lose all or a substantial portion of the money that you pay for our common stock.
Risk Related to our Company and our Business
Risks Related to Our Financial Position and Need for Capital
We are a clinical stage biopharmaceutical company with a limited operating history.
We are a clinical stage biopharmaceutical company with a limited operating history. We must obtain FDA clearance of our Investigational New Drug applications, or INDs, before clinical trials can commence, and must receive regulatory approval of our New Drug Applications, or NDAs, before commercial sales of a product can commence. The likelihood of success of our business plan must be considered in light of the problems, substantial expenses, difficulties, complications and delays frequently encountered in connection with developing and expanding early-stage businesses and the regulatory and competitive environment in which we operate. Biopharmaceutical product development is a highly speculative undertaking, involves a substantial degree of risk and is a capital-intensive business.
Accordingly, you should consider our prospects in light of the costs, uncertainties, delays and difficulties frequently encountered by companies in the early stages of development, especially clinical biopharmaceutical companies such as ours. Potential investors should carefully consider the risks and uncertainties that a company with a limited operating history will face. In particular, potential investors should consider that we cannot assure you that we will be able to:
| | receive FDA approval of INDs for commencing our clinical trials; |
| | successfully implement or execute our current business plan, or that our business plan is sound; |
| | successfully complete clinical trials and obtain regulatory approval for the marketing of Resunab; |
| | successfully manufacture our clinical product and establish commercial drug supply; |
| | secure market exclusivity and/or adequate intellectual property protection for Resunab; |
| | attract and retain an experienced management and advisory team; |
| | secure acceptance of Resunab in the medical community and with third party payors and consumers; |
| | launch commercial sales of Resunab, whether alone or in collaboration with others; and |
| | raise sufficient funds in the capital markets to effectuate our business plan including clinical development, regulatory approval and commercialization for Resunab. |
If we cannot successfully execute any one of the foregoing, our business may not succeed and your investment will be adversely affected.
We have incurred operating losses in each year since our inception and expect to continue to incur substantial losses for the foreseeable future. We may never become profitable or, if achieved, be able to sustain profitability.
We expect to incur substantial expenses without corresponding revenues unless and until we are able to obtain regulatory approval and successfully commercialize Resunab. We have been engaged in developing Resunab since 2009. To date, we have not generated any revenue from Resunab and we expect to incur significant expense to complete our clinical program for Resunab in the United States and elsewhere. We may never be able to obtain regulatory approval for the marketing of Resunab in any indication in the United States or internationally. Even if we are able to commercialize Resunab or any other product candidate, there can be no assurance that we will generate significant revenues or ever achieve profitability. Our net losses for the years ended December 31, 2014 and December 31, 2013 were approximately $2,540,000 and approximately $602,000, respectively. As of December 31, 2014, we had an accumulated deficit of approximately $4,427,000.
10
Table of Contents
Assuming we obtain FDA approval for Resunab, which we do not expect until 2018 at the earliest, we expect that our research and development expenses will continue to increase as we advance to clinical trials for indications for the treatment of cystic fibrosis and scleroderma. We may elect to pursue FDA approval for Resunab in other indications, which will result in significant additional research and development expenses. As a result, we expect to continue to incur substantial losses for the foreseeable future, and these losses will increase. We are uncertain when or if we will be able to achieve or sustain profitability. If we achieve profitability in the future, we may not be able to sustain profitability in subsequent periods. Failure to become and remain profitable would impair our ability to sustain operations and adversely affect the price of our common stock and our ability to raise capital.
Our cash or cash equivalents will only fund our operations for a limited time and we will need to raise additional capital to support our development and commercialization efforts.
We are currently operating at a loss and expect our operating costs will increase significantly as we incur costs related to the clinical trials for Resunab. We believe that our cash on hand will be sufficient to fund our operations through at least the end of 2015.
We do not currently have any arrangements or credit facilities in place as a source of funds, and there can be no assurance that we will be able to raise sufficient additional capital on acceptable terms, or at all. We may seek additional capital through a combination of private and public equity offerings, debt financings and strategic collaborations. Debt financing, if obtained, may involve agreements that include covenants limiting or restricting our ability to take specific actions, such as incurring additional debt, and could increase our expenses and require that our assets secure such debt.
Equity financing, if obtained, could result in dilution to our then existing stockholders and/or require such stockholders to waive certain rights and preferences. If such financing is not available on satisfactory terms, or is not available at all, we may be required to delay, scale back or eliminate the development of business opportunities and our operations and financial condition may be materially adversely affected. We may have difficulty obtaining such financing while certain outstanding payments of our current debt remain in default. We can provide no assurances that any additional sources of financing will be available to us on favorable terms, if at all. In addition, if we are unable to secure sufficient capital to fund our operations, we might have to enter into strategic collaborations that could require us to share commercial rights to Resunab with third parties in ways that we currently do not intend or on terms that may not be favorable to us. If we choose to pursue additional indications and/or geographies for Resunab or otherwise expand more rapidly than we presently anticipate we may also need to raise additional capital sooner than expected.
Risks Related to Product Development, Regulatory Approval, Manufacturing and Commercialization
We depend entirely on the success of Resunab, which has not yet demonstrated efficacy in Phase II clinical trials. If we are unable to generate revenues from Resunab, our ability to create stockholder value will be limited.
Our only product candidate currently is Resunab, which has successfully completed Phase I safety studies but has not yet entered into Phase II clinical studies for cystic fibrosis or scleroderma. We do not generate revenues from any FDA approved drug products and have no other product candidates in development. We submitted an IND to the FDA seeking approval to initiate Phase IIa clinical trials in humans in the United States for the treatment of scleroderma on February 5, 2015. On March 5, 2015, we received FDA authorization to initiate the scleroderma clinical trial. We must submit an additional clinical protocol to the FDA for the Resunab IND before we can commence Phase IIa clinical trials for cystic fibrosis, and may not commence human clinical trials in scleroderma until the second quarter of 2015 at the earliest, and do not intend to submit to the FDA the clinical protocol for cystic fibrosis or commence clinical studies until the second quarter of 2015. The FDA may reject the clinical protocol for cystic fibrosis at any time during the 30 day period following the IND submission. If the clinical protocol for cystic fibrosis is rejected, the time in which we expect to commence our Phase II clinical program for cystic fibrosis will be extended and such extension will increase our expenses and increase our need for additional capital. Moreover, there is no guarantee that our Phase II clinical trials will be successful or that we will continue with clinical studies to support an approval from the FDA for any indication. We note that most drug candidates never reach the clinical development stage and even those that do reach clinical development have only a small chance of successfully completing clinical development and gaining regulatory approval. Therefore, our business currently depends entirely on the successful development, regulatory approval and commercialization of Resunab, which may never occur.
If we are not able to obtain any required regulatory approvals for Resunab, we will not be able to commercialize our only product candidate and our ability to generate revenue will be limited.
We must successfully complete clinical trials for Resunab before we can apply for marketing approval. Even if we complete our clinical trials, it does not assure FDA approval. Our Phase IIa clinical trials may be unsuccessful, which would materially harm our business. Even if these Phase IIa clinical trials are successful, we are required to conduct additional clinical trials to establish Resunabs safety and efficacy, before a New Drug Application, or NDA, can be filed with the FDA for marketing approval of Resunab.
11
Table of Contents
Clinical testing is expensive, is difficult to design and implement, can take many years to complete and is uncertain as to outcome. Success in early phases of pre-clinical and clinical trials does not ensure that later clinical trials will be successful, and interim results of a clinical trial do not necessarily predict final results. A failure of one or more of our clinical trials can occur at any stage of testing. We may experience numerous unforeseen events during, or as a result of, the clinical trial process that could delay or prevent our ability to receive regulatory approval or commercialize Resunab. The research, testing, manufacturing, labeling, packaging, storage, approval, sale, marketing, advertising and promotion, pricing, export, import and distribution of drug products are subject to extensive regulation by the FDA and other regulatory authorities in the United States and other countries, which regulations differ from country to country. We are not permitted to market Resunab as a prescription pharmaceutical product in the United States until we receive approval of an NDA from the FDA, or in any foreign countries until we receive the requisite approval from such countries. In the United States, the FDA generally requires the completion of clinical trials of each drug to establish its safety and efficacy and extensive pharmaceutical development to ensure its quality before an NDA is approved. Regulatory authorities in other jurisdictions impose similar requirements. Of the large number of drugs in development, only a small percentage result in the submission of an NDA to the FDA and even fewer are eventually approved for commercialization. We have never submitted an NDA to the FDA or comparable applications to other regulatory authorities. If our development efforts for Resunab, including regulatory approval, are not successful for its planned indications, or if adequate demand for Resunab is not generated, our business will be harmed.
Our success depends on the receipt of regulatory approval and the issuance of such regulatory approvals is uncertain and subject to a number of risks, including the following:
| | the FDA or comparable foreign regulatory authorities or institutional review boards, or IRBs, may disagree with the design or implementation of our clinical trials; |
| | we may not be able to provide acceptable evidence of Resunabs safety and efficacy; |
| | the results of our clinical trials may not be satisfactory or may not meet the level of statistical or clinical significance required by the FDA, European Medicines Agency, or EMA, or other comparable foreign regulatory authorities for marketing approval; |
| | the dosing of Resunab in a particular clinical trial may not be at an optimal level; |
| | patients in our clinical trials may suffer adverse effects for reasons that may or may not be related to Resunab; |
| | the data collected from clinical trials may not be sufficient to support the submission of an NDA or other submission or to obtain regulatory approval in the United States or elsewhere; |
| | the FDA or comparable foreign regulatory authorities may fail to approve the manufacturing processes or facilities of third- party manufacturers with which we contract for clinical and commercial supplies; and |
| | the approval policies or regulations of the FDA or comparable foreign regulatory authorities may significantly change in a manner rendering our clinical data insufficient for approval. |
Failure to obtain regulatory approval for Resunab for the foregoing or any other reasons will prevent us from commercializing this product candidate as a prescription product, and our ability to generate revenue will be materially impaired. We cannot guarantee that regulators will agree with our assessment of the results of the clinical trials we intend to conduct in the future or that such trials will be successful. The FDA, EMA and other regulators have substantial discretion in the approval process and may refuse to accept any application or may decide that our data is insufficient for approval and require additional clinical trials, or pre-clinical or other studies. In addition, varying interpretations of the data obtained from pre-clinical and clinical testing could delay, limit or prevent regulatory approval of a product candidate.
We are a clinical stage company and we have not submitted an NDA or received regulatory approval to market Resunab in any jurisdiction. We have only limited experience in filing the applications necessary to gain regulatory approvals and expect to rely on consultants and third party contract research organizations, or CROs, with expertise in this area to assist us in this process. Securing FDA approval requires the submission of pre-clinical, clinical, and/or pharmacokinetic data, information about product manufacturing processes and inspection of facilities and supporting information to the FDA for each therapeutic indication to establish a product candidates safety and efficacy for each indication. Resunab may prove to have undesirable or unintended side effects, toxicities or other characteristics that may preclude our obtaining regulatory approval or prevent or limit commercial use with respect to one or all intended indications.
The process of obtaining regulatory approvals is expensive, often takes many years, if approval is obtained at all, and can vary substantially based upon, among other things, the type, complexity and novelty of the product candidates involved, the jurisdiction in which regulatory approval is sought and the substantial discretion of the regulatory authorities. Changes in the regulatory approval policy during the development period, changes in or the enactment of additional statutes or regulations, or changes in regulatory review for a submitted product application may cause delays in the approval or rejection of an application. Regulatory approval obtained in one jurisdiction does not
12
Table of Contents
necessarily mean that a product candidate will receive regulatory approval in all jurisdictions in which we may seek approval, but the failure to obtain approval in one jurisdiction may negatively impact our ability to seek approval in a different jurisdiction. Failure to obtain regulatory marketing approval for Resunab in any indication will prevent us from commercializing the product candidate, and our ability to generate revenue will be materially impaired.
Resunab is our only product candidate in development. If we fail to successfully commercialize Resunab, we may need to acquire additional product candidates and our business will be adversely affected.
We have never commercialized any product candidates and do not have any other compounds in pre-clinical testing, lead optimization or lead identification stages beyond Resunab. We cannot be certain that Resunab will prove to be sufficiently effective and safe to meet applicable regulatory standards for any indication. If we fail to successfully commercialize Resunab as a treatment for cystic fibrosis, scleroderma or any other indication, whether as a stand-alone therapy or in combination with other treatments, our business would be adversely affected.
Even if we receive regulatory approval for Resunab, we still may not be able to successfully commercialize this product, and the revenue that we generate from its sales, if any, may be limited.
If approved for marketing, the commercial success of Resunab will depend upon its acceptance by the medical community, including physicians, patients and health care payors. The degree of market acceptance of Resunab will depend on a number of factors, including:
| | demonstration of clinical safety and efficacy; |
| | relative convenience, pill burden and ease of administration; |
| | the prevalence and severity of any adverse effects; |
| | the willingness of physicians to prescribe Resunab and of the target patient population to try new therapies; |
| | efficacy of Resunab compared to competing products; |
| | the introduction of any new products that may in the future become available to treat indications for which Resunab may be approved; |
| | new procedures or methods of treatment that may reduce the incidences of any of the indications in which Resunab may show utility; |
| | pricing and cost-effectiveness; |
| | the inclusion or omission of Resunab in applicable treatment guidelines; |
| | the effectiveness of our or any future collaborators sales and marketing strategies; |
| | limitations or warnings contained in FDA-approved labeling; |
| | our ability to obtain and maintain sufficient third-party coverage or reimbursement from government health care programs, including Medicare and Medicaid, private health insurers and other third-party payors; and |
| | the willingness of patients to pay out-of-pocket in the absence of third-party coverage or reimbursement. |
If Resunab is approved, but does not achieve an adequate level of acceptance by physicians, health care payors and patients, we may not generate sufficient revenue and we may not be able to achieve or sustain profitability. Our efforts to educate the medical community and third-party payors on the benefits of Resunab may require significant resources and may never be successful.
In addition, even if we obtain regulatory approvals, the timing or scope of any approvals may prohibit or reduce our ability to commercialize Resunab successfully. For example, if the approval process takes too long, we may miss market opportunities and give other companies the ability to develop competing products or establish market dominance. Any regulatory approval we ultimately obtain may be limited or subject to restrictions or post-approval commitments that render Resunab not commercially viable. For example, regulatory authorities may approve Resunab for fewer or more limited indications than we request, may not approve the price we intend to charge for Resunab, may grant approval contingent on the performance of costly post-marketing clinical trials, or may approve Resunab with a label that does not include the labeling claims necessary or desirable for the successful commercialization of that indication. Further, the FDA or comparable foreign regulatory authorities may place conditions on approvals, such as risk management plans and a Risk Evaluation and Mitigation Strategy, or REMS, to assure the safe use of the drug. If the FDA concludes a REMS is needed, the sponsor of the NDA must submit a proposed REMS; the FDA will not approve the NDA without an approved REMS, if required. A REMS could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. The FDA may also require a REMS for an approved product when new safety information emerges. Any of these
13
Table of Contents
limitations on approval or marketing could restrict the commercial promotion, distribution, prescription or dispensing of Resunab. Moreover, product approvals may be withdrawn for non-compliance with regulatory standards or if problems occur following the initial marketing of the product. Any of the foregoing scenarios could materially harm the commercial success of Resunab.
Even if we obtain marketing approval for Resunab, we will be subject to ongoing obligations and continued regulatory review, which may result in significant additional expense. Additionally, Resunab could be subject to labeling and other restrictions and withdrawal from the market and we may be subject to penalties if we fail to comply with regulatory requirements or if we experience unanticipated problems with Resunab.
Even if we obtain United States regulatory approval of Resunab for an indication, the FDA may still impose significant restrictions on its indicated uses or marketing or the conditions of approval, or impose ongoing requirements for potentially costly and time-consuming post-approval studies, including Phase IV clinical trials, and post-market surveillance to monitor safety and efficacy. Resunab will also be subject to ongoing regulatory requirements governing the manufacturing, labeling, packaging, storage, distribution, safety surveillance, advertising, promotion, recordkeeping and reporting of adverse events and other post-market information. These requirements include registration with the FDA, as well as continued compliance with current Good Clinical Practices regulations, or cGCPs, for any clinical trials that we conduct post-approval. In addition, manufacturers of drug products and their facilities are subject to continual review and periodic inspections by the FDA and other regulatory authorities for compliance with current Good Manufacturing Practices, or cGMP, requirements relating to quality control, quality assurance and corresponding maintenance of records and documents.
The FDA has the authority to require a risk evaluation and mitigation strategy, or REMS, as part of an NDA or after approval, which may impose further requirements or restrictions on the distribution or use of an approved drug, such as limiting prescribing to certain physicians or medical centers that have undergone specialized training, limiting treatment to patients who meet certain safe-use criteria or requiring patient testing, monitoring and/or enrollment in a registry.
With respect to sales and marketing activities by us or any future partner, advertising and promotional materials must comply with FDA rules in addition to other applicable federal, state and local laws in the United States and similar legal requirements in other countries. In the United States, the distribution of product samples to physicians must comply with the requirements of the U.S. Prescription Drug Marketing Act. Application holders must obtain FDA approval for product and manufacturing changes, depending on the nature of the change. We may also be subject, directly or indirectly through our customers and partners, to various fraud and abuse laws, including, without limitation, the U.S. Anti-Kickback Statute, U.S. False Claims Act, and similar state laws, which impact, among other things, our proposed sales, marketing, and scientific/educational grant programs. If we participate in the U.S. Medicaid Drug Rebate Program, the Federal Supply Schedule of the U.S. Department of Veterans Affairs, or other government drug programs, we will be subject to complex laws and regulations regarding reporting and payment obligations. All of these activities are also potentially subject to U.S. federal and state consumer protection and unfair competition laws. Similar requirements exist in many of these areas in other countries.
In addition, if Resunab is approved for an indication, our product labeling, advertising and promotion would be subject to regulatory requirements and continuing regulatory review. The FDA strictly regulates the promotional claims that may be made about prescription products. In particular, a product may not be promoted for uses that are not approved by the FDA as reflected in the products approved labeling. If we receive marketing approval for Resunab, physicians may nevertheless legally prescribe our products to their patients in a manner that is inconsistent with the approved label. If we are found to have promoted such off-label uses, we may become subject to significant liability and government fines. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses by a company, and any company that is found to have improperly promoted off-label uses may be subject to significant sanctions. The federal government has levied large civil and criminal fines against companies for alleged improper promotion and has enjoined several companies from engaging in off-label promotion. The FDA has also requested that companies enter into consent decrees of permanent injunctions under which specified promotional conduct is changed or curtailed.
If we or a regulatory agency discover previously unknown problems with a product, such as adverse events of unanticipated severity or frequency, problems with the facility where the product is manufactured, or if we or our manufacturers fail to comply with applicable regulatory requirements, we may be subject to the following administrative or judicial sanctions:
| | restrictions on the marketing or manufacturing of the product, withdrawal of the product from the market, or voluntary or mandatory product recalls; |
| | issuance of warning letters or untitled letters; |
| | clinical holds; |
| | injunctions or the imposition of civil or criminal penalties or monetary fines; |
| | suspension or withdrawal of regulatory approval; |
14
Table of Contents
| | suspension of any ongoing clinical trials; |
| | refusal to approve pending applications or supplements to approved applications filed by us, or suspension or revocation of product license approvals; |
| | suspension or imposition of restrictions on operations, including costly new manufacturing requirements; or |
| | product seizure or detention or refusal to permit the import or export of product. |
The occurrence of any event or penalty described above may inhibit our ability to commercialize Resunab and generate revenue. Adverse regulatory action, whether pre- or post-approval, can also potentially lead to product liability claims and increase our product liability exposure.
We currently have no sales and marketing organization. If we are unable to secure a sales and marketing partner or establish satisfactory sales and marketing capabilities, we may not successfully commercialize Resunab.
At present, we have no sales or marketing personnel. In order to commercialize products that are approved for commercial sales, we must either collaborate with third parties that have such commercial infrastructure or develop our own sales and marketing infrastructure. If we are not successful entering into appropriate collaboration arrangements, or recruiting sales and marketing personnel or in building a sales and marketing infrastructure, we will have difficulty successfully commercializing Resunab, which would adversely affect our business, operating results and financial condition.
We may not be able to enter into collaboration agreements on terms acceptable to us or at all. In addition, even if we enter into such relationships, we may have limited or no control over the sales, marketing and distribution activities of these third parties. Our future revenues may depend heavily on the success of the efforts of these third parties. If we elect to establish a sales and marketing infrastructure we may not realize a positive return on this investment. In addition, we will have to compete with established and well-funded pharmaceutical and biotechnology companies to recruit, hire, train and retain sales and marketing personnel. Factors that may inhibit our efforts to commercialize Resunab without strategic partners or licensees include:
| | our inability to recruit and retain adequate numbers of effective sales and marketing personnel; |
| | the inability of sales personnel to obtain access to or persuade adequate numbers of physicians to prescribe Resunab; |
| | the lack of complementary products to be offered by sales personnel, which may put us at a competitive disadvantage relative to companies with more extensive product lines; and |
| | unforeseen costs and expenses associated with creating an independent sales and marketing organization. |
We face competition from other biotechnology and pharmaceutical companies and our operating results will suffer if we fail to compete effectively.
The biotechnology and pharmaceutical industries are intensely competitive and subject to rapid and significant technological change. We have competitors in a number of jurisdictions, many of which have substantially greater name recognition, commercial infrastructures and financial, technical and personnel resources than we have. Established competitors may invest heavily to quickly discover and develop novel compounds that could make Resunab obsolete or uneconomical. Any new product that competes with an approved product may need to demonstrate compelling advantages in efficacy, cost, convenience, tolerability and safety to be commercially successful. Other competitive factors, including generic competition, could force us to lower prices or could result in reduced sales. In addition, new products developed by others could emerge as competitors to Resunab. If we are not able to compete effectively against our current and future competitors, our business will not grow and our financial condition and operations will suffer.
Our potential competitors both in the United States and Europe include companies developing and/or marketing drugs for cystic fibrosis, including Vertex, N30 Pharmaceuticals LLC and PTC Therapeutics (NasdaqGS: PTCT), as well as companies working in the scleroderma field, including Bristol-Myers Squibb and Sanofi.
Recently enacted and future legislation may increase the difficulty and cost for us to obtain marketing approval of and commercialize Resunab and affect the prices we may obtain.
In the United States and some foreign jurisdictions, there have been a number of legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay marketing approval for Resunab, restrict or regulate post-approval activities and affect our ability to profitably sell Resunab. Legislative and regulatory proposals have been made to expand post-approval requirements and restrict sales and promotional activities for pharmaceutical products. We do not know whether additional legislative changes
15
Table of Contents
will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of Resunab, if any, may be. In addition, increased scrutiny by the U.S. Congress of the FDAs approval process may significantly delay or prevent marketing approval, as well as subject us to more stringent product labeling and post-marketing testing and other requirements.
In the United States, the Medicare Modernization Act, or MMA, changed the way Medicare covers and pays for pharmaceutical products. The legislation expanded Medicare coverage for drug purchases by the elderly and introduced a new reimbursement methodology based on average sales prices for drugs. In addition, this legislation authorized Medicare Part D prescription drug plans to use formularies where they can limit the number of drugs that will be covered in any therapeutic class. As a result of this legislation and the expansion of federal coverage of drug products, we expect that there will be additional pressure to contain and reduce costs. These cost reduction initiatives and other provisions of this legislation could decrease the coverage and price that we receive for Resunab and could seriously harm our business. While the MMA applies only to drug benefits for Medicare beneficiaries, private payors often follow Medicare coverage policy and payment limitations in setting their own reimbursement rates, and any reduction in reimbursement that results from the MMA may result in a similar reduction in payments from private payors.
In March 2010, President Obama signed into law the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Affordability Reconciliation Act of 2010 or, collectively, the Health Care Reform Law, a sweeping law intended to broaden access to health insurance, reduce or constrain the growth of healthcare spending, enhance remedies against fraud and abuse, add new transparency requirements for healthcare and health insurance industries, impose new taxes and fees on the health industry and impose additional health policy reforms. Effective October 1, 2010, the Health Care Reform Law revised the definition of average manufacturer price for reporting purposes, which could increase the amount of Medicaid drug rebates to states. Further, the new law imposed a significant annual fee on companies that manufacture or import branded prescription drug products. Substantial new provisions affecting compliance have also been enacted, which may require us to modify our business practices with healthcare practitioners, and incur substantial costs to ensure compliance.
Despite initiatives to invalidate the Health Care Reform Law, at this time it appears the implementation of the Health Care Reform Law will continue. We will not know the full effects of the Health Care Reform Law until applicable federal and state agencies issue regulations or guidance under the new law. Although it is too early to determine the effect of the Health Care Reform Law, the new law appears likely to continue the pressure on pharmaceutical pricing, especially under the Medicare program, and may also increase our regulatory burdens and operating costs.
In addition, other legislative changes have been proposed and adopted in the United States since the Health Care Reform Law was enacted. On August 2, 2011, the Budget Control Act of 2011 among other things, created measures for spending reductions by Congress. A Joint Select Committee on Deficit Reduction, tasked with recommending a targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, was unable to reach required goals, thereby triggering the legislations automatic reduction to several government programs. This includes aggregate reductions to Medicare payments to providers of up to 2% per fiscal year, starting in 2013. On January 2, 2013, President Obama signed into law the American Taxpayer Relief Act of 2012, or the ATRA, which delayed for another two months the budget cuts mandated by these sequestration provisions of the Budget Control Act of 2011. The ATRA, among other things, also reduced Medicare payments to several providers, including hospitals, imaging centers and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. We expect that additional federal healthcare reform measures will be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, and in turn could significantly reduce the projected value of certain development projects and reduce our profitability.
Our future growth depends, in part, on our ability to penetrate foreign markets, where we would be subject to additional regulatory burdens and other risks and uncertainties.
Our future profitability will depend, in part, on our ability to commercialize Resunab in foreign markets for which we intend to rely on collaborations with third parties. If we commercialize Resunab in foreign markets, we would be subject to additional risks and uncertainties, including:
| | our customers ability to obtain reimbursement for Resunab in foreign markets; |
| | our inability to directly control commercial activities because we are relying on third parties; |
| | the burden of complying with complex and changing foreign regulatory, tax, accounting and legal requirements; |
| | different medical practices and customs in foreign countries affecting acceptance in the marketplace; |
| | import or export licensing requirements; |
| | longer accounts receivable collection times; |
16
Table of Contents
| | longer lead times for shipping; |
| | language barriers for technical training; |
| | reduced protection of intellectual property rights in some foreign countries; |
| | foreign currency exchange rate fluctuations; and |
| | the interpretation of contractual provisions governed by foreign laws in the event of a contract dispute. |
Foreign sales of Resunab could also be adversely affected by the imposition of governmental controls, political and economic instability, trade restrictions and changes in tariffs, any of which may adversely affect our results of operations.
If we market Resunab in a manner that violates healthcare fraud and abuse laws, or if we violate government price reporting laws, we may be subject to civil or criminal penalties.
The FDA enforces laws and regulations which require that the promotion of pharmaceutical products be consistent with the approved prescribing information. While physicians may prescribe an approved product for a so-called off label use, it is unlawful for a pharmaceutical company to promote its products in a manner that is inconsistent with its approved label and any company which engages in such conduct can subject that company to significant liability. Similarly, industry codes in the European Union and other foreign jurisdictions prohibit companies from engaging in off-label promotion and regulatory agencies in various countries enforce violations of the code with civil penalties. While we intend to ensure that our promotional materials are consistent with our label, regulatory agencies may disagree with our assessment and may issue untitled letters, warning letters or may institute other civil or criminal enforcement proceedings. In addition to FDA restrictions on marketing of pharmaceutical products, several other types of state and federal healthcare fraud and abuse laws have been applied in recent years to restrict certain marketing practices in the pharmaceutical industry. These laws include the U.S. Anti-Kickback Statute, U.S. False Claims Act and similar state laws. Because of the breadth of these laws and the narrowness of the safe harbors, it is possible that some of our business activities could be subject to challenge under one or more of these laws.
The U.S. Anti-Kickback Statute prohibits, among other things, knowingly and willfully offering, paying, soliciting or receiving remuneration to induce, or in return for, purchasing, leasing, ordering or arranging for the purchase, lease or order of any healthcare item or service reimbursable under Medicare, Medicaid or other federally financed healthcare programs. This statute has been interpreted broadly to apply to arrangements between pharmaceutical manufacturers on the one hand and prescribers, purchasers and formulary managers on the other. Although there are several statutory exemptions and regulatory safe harbors protecting certain common activities from prosecution, the exemptions and safe harbors are drawn narrowly, and practices that involve remuneration intended to induce prescribing, purchasing or recommending may be subject to scrutiny if they do not qualify for an exemption or safe harbor. Our practices may not, in all cases, meet all of the criteria for safe harbor protection from anti-kickback liability. Moreover, recent health care reform legislation has strengthened these laws. For example, the Health Care Reform Law, among other things, amends the intent requirement of the U.S. Anti-Kickback Statute and criminal health care fraud statutes; a person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it. In addition, the Health Care Reform Law provides that the government may assert that a claim including items or services resulting from a violation of the U.S. Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the U.S. False Claims Act. Federal false claims laws prohibit any person from knowingly presenting, or causing to be presented, a false claim for payment to the federal government or knowingly making, or causing to be made, a false statement to get a false claim paid.
Over the past few years, pharmaceutical and other healthcare companies have been prosecuted under these laws for a variety of alleged promotional and marketing activities, such as: allegedly providing free trips, free goods, sham consulting fees and grants and other monetary benefits to prescribers; reporting to pricing services inflated average wholesale prices that were then used by federal programs to set reimbursement rates; engaging in off-label promotion that caused claims to be submitted to Medicare or Medicaid for non-covered, off-label uses; and submitting inflated best price information to the Medicaid Rebate Program to reduce liability for Medicaid rebates. Most states also have statutes or regulations similar to the U.S. Anti-Kickback Statute and the U.S. False Claims Act, which apply to items and services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of the payor. Sanctions under these federal and state laws may include substantial civil monetary penalties, exclusion of a manufacturers products from reimbursement under government programs, substantial criminal fines and imprisonment.
We are, and will be, completely dependent on third parties to manufacture Resunab, and our commercialization of Resunab could be halted, delayed or made less profitable if those third parties fail to obtain manufacturing approval from the FDA or comparable foreign regulatory authorities, fail to provide us with sufficient quantities of Resunab or fail to do so at acceptable quality levels or prices.
We do not currently have, nor do we plan to acquire, the capability or infrastructure to manufacture the active pharmaceutical ingredient, or API, in Resunab for use in our clinical trials or for commercial product, if any. In addition, we do not have the capability to encapsulate Resunab as a finished drug product for commercial distribution. As a result, we will be obligated to rely on contract manufacturers, if and when Resunab is approved for commercialization. We have not entered into an agreement with any contract manufacturers for commercial supply and may not be able to engage a contract manufacturer for commercial supply of Resunab on favorable terms to us, or at all.
17
Table of Contents
The facilities used by our contract manufacturers to manufacture Resunab must be approved by the FDA pursuant to inspections that will be conducted after we submit our NDA to the FDA. We do not control the manufacturing process of, and are completely dependent on, our contract manufacturing partners for compliance with cGMPs for manufacture of both active drug substances and finished drug products. These cGMP regulations cover all aspects of the manufacturing, testing, quality control and record keeping relating to Resunab. If our contract manufacturers cannot successfully manufacture material that conforms to our specifications and the strict regulatory requirements of the FDA or others, they will not be able to secure and/or maintain regulatory approval for their manufacturing facilities. If the FDA or a comparable foreign regulatory authority does not approve these facilities for the manufacture of Resunab or if it withdraws any such approval in the future, we may need to find alternative manufacturing facilities, which would significantly impact our ability to develop, obtain regulatory approval for or market Resunab, if approved.
Our contract manufacturers will be subject to ongoing periodic unannounced inspections by the FDA and corresponding state and foreign agencies for compliance with cGMPs and similar regulatory requirements. We will not have control over our contract manufacturers compliance with these regulations and standards. Failure by any of our contract manufacturers to comply with applicable regulations could result in sanctions being imposed on us, including fines, injunctions, civil penalties, failure to grant approval to market Resunab, delays, suspensions or withdrawals of approvals, operating restrictions and criminal prosecutions, any of which could significantly and adversely affect our business. In addition, we will not have control over the ability of our contract manufacturers to maintain adequate quality control, quality assurance and qualified personnel. Failure by our contract manufacturers to comply with or maintain any of these standards could adversely affect our ability to develop, obtain regulatory approval for or market Resunab.
If for any reason, these third parties are unable or unwilling to perform, we may not be able to terminate our agreements with them, and we may not be able to locate alternative manufacturers or formulators or enter into favorable agreements with them and we cannot be certain that any such third parties will have the manufacturing capacity to meet future requirements. If these manufacturers or any alternate manufacturer of finished drug product experiences any significant difficulties in its respective manufacturing processes for our API or finished Resunab product or should cease doing business with us, we could experience significant interruptions in the supply of Resunab or may not be able to create a supply of Resunab at all. Were we to encounter manufacturing issues, our ability to produce a sufficient supply of Resunab might be negatively affected. Our inability to coordinate the efforts of our third party manufacturing partners, or the lack of capacity available at our third party manufacturing partners, could impair our ability to supply Resunab at required levels. Because of the significant regulatory requirements that we would need to satisfy in order to qualify a new bulk or finished product manufacturer, if we face these or other difficulties with our current manufacturing partners, we could experience significant interruptions in the supply of Resunab if we decided to transfer the manufacture of Resunab to one or more alternative manufacturers in an effort to deal with the difficulties.
Any manufacturing problem or the loss of a contract manufacturer could be disruptive to our operations and result in lost sales. Additionally, we rely on third parties to supply the raw materials needed to manufacture our potential products. Any reliance on suppliers may involve several risks, including a potential inability to obtain critical materials and reduced control over production costs, delivery schedules, reliability and quality. Any unanticipated disruption to a future contract manufacturer caused by problems at suppliers could delay shipment of Resunab, increase our cost of goods sold and result in lost sales.
We cannot guarantee that our manufacturing and supply partners will be able to reduce the costs of commercial scale manufacturing of Resunab over time. If the commercial-scale manufacturing costs of Resunab are higher than expected, these costs may significantly impact our operating results. In order to reduce costs, we may need to develop and implement process improvements. However, in order to do so, we will need, from time to time, to notify or make submissions with regulatory authorities, and the improvements may be subject to approval by such regulatory authorities. We cannot be sure that we will receive these necessary approvals or that these approvals will be granted in a timely fashion. We also cannot guarantee that we will be able to enhance and optimize output in our commercial manufacturing process. If we cannot enhance and optimize output, we may not be able to reduce our costs over time.
We expect that we will rely on third parties to conduct clinical trials for Resunab. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval for or commercialize Resunab and our business would be substantially harmed.
We expect to enter into agreements with third-party CROs to conduct and manage our clinical programs including contracting with clinical sites to perform our clinical studies. We plan to rely heavily on these parties for execution of clinical studies for Resunab and will control only certain aspects of their activities. Nevertheless, we will be responsible for ensuring that each of our studies is conducted in accordance with the applicable protocol, legal, regulatory and scientific standards, and our reliance on CROs and clinical sites will not relieve us of our regulatory responsibilities. We and our CROs will be required to comply with cGCPs, which are regulations and guidelines enforced by the FDA, the Competent Authorities of the Member States of the European Economic Area and comparable foreign regulatory authorities
18
Table of Contents
for any products in clinical development. The FDA enforces these cGCP regulations through periodic inspections of trial sponsors, principal investigators and trial sites. If we or our CROs fail to comply with applicable cGCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot assure you that, upon inspection, the FDA will determine that any of our clinical trials comply with cGCPs. In addition, our clinical trials must be conducted with products produced under cGMP regulations and will require a large number of test subjects. Our failure or the failure of our CROs or clinical sites to comply with these regulations may require us to repeat clinical trials, which would delay the regulatory approval process and could also subject us to enforcement action up to and including civil and criminal penalties.
Although we intend to design the clinical trials for Resunab in consultation with CROs, we expect that the CROs will manage all of the clinical trials conducted at contracted clinical sites. As a result, many important aspects of our drug development programs would be outside of our direct control. In addition, the CROs and clinical sites may not perform all of their obligations under arrangements with us or in compliance with regulatory requirements. If the CROs or clinical sites do not perform clinical trials in a satisfactory manner, breach their obligations to us or fail to comply with regulatory requirements, the development and commercialization of Resunab for the subject indication may be delayed or our development program materially and irreversibly harmed. We cannot control the amount and timing of resources these CROs and clinical sites will devote to our program or Resunab. If we are unable to rely on clinical data collected by our CROs, we could be required to repeat, extend the duration of, or increase the size of our clinical trials, which could significantly delay commercialization and require significantly greater expenditures.
If any of our relationships with these third-party CROs or clinical sites terminate, we may not be able to enter into arrangements with alternative CROs or clinical sites. If CROs do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols, regulatory requirements or for other reasons, any such clinical trials may be extended, delayed or terminated, and we may not be able to obtain regulatory approval for or successfully commercialize Resunab. As a result, our financial results and the commercial prospects for Resunab would be harmed, our costs could increase and our ability to generate revenue could be delayed.
Any termination or suspension of or delays in the commencement or completion of any necessary studies of Resunab for any indications could result in increased costs to us, delay or limit our ability to generate revenue and adversely affect our commercial prospects.
The commencement and completion of clinical studies can be delayed for a number of reasons, including delays related to:
| | the FDA failing to grant permission to proceed and placing the clinical study on hold; |
| | subjects failing to enroll or remain in our trials at the rate we expect; |
| | a facility manufacturing Resunab being ordered by the FDA or other government or regulatory authorities to temporarily or permanently shut down due to violations of cGMP requirements or other applicable requirements, or cross-contaminations of product in the manufacturing process; |
| | any changes to our manufacturing process that may be necessary or desired; |
| | subjects choosing an alternative treatment for the indications for which we are developing Resunab, or participating in competing clinical studies; |
| | subjects experiencing severe or unexpected drug-related adverse effects; |
| | reports of similar technologies and products raising safety and/or efficacy concerns; |
| | third-party clinical investigators losing their license or permits necessary to perform our clinical trials, not performing our clinical trials on our anticipated schedule or employing methods consistent with the clinical trial protocol, cGCP requirements, or other third parties not performing data collection and analysis in a timely or accurate manner; |
| | inspections of clinical study sites by the FDA or IRBs finding regulatory violations that require us to undertake corrective action, result in suspension or termination of one or more sites or the imposition of a clinical hold on the entire study, or that prohibit us from using some or all of the data in support of our marketing applications; |
| | third-party contractors becoming debarred or suspended or otherwise penalized by the FDA or other government or regulatory authorities for violations of regulatory requirements, in which case we may need to find a substitute contractor, and we may not be able to use some or any of the data produced by such contractors in support of our marketing applications; |
| | one or more IRBs refusing to approve, suspending or terminating the study at an investigational site precluding enrollment of additional subjects, or withdrawing its approval of the trial; reaching agreement on acceptable terms with prospective CROs and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites; |
19
Table of Contents
| | deviations of the clinical sites from trial protocols or dropping out of a trial; |
| | adding new clinical trial sites; |
| | the inability of the CRO to execute any clinical trials for any reason; and |
| | government or regulatory delays or clinical holds requiring suspension or termination of a trial. |
Product development costs for Resunab will increase if we have delays in testing or approval or if we need to perform more or larger clinical studies than planned. Additionally, changes in regulatory requirements and policies may occur and we may need to amend study protocols to reflect these changes. Amendments may require us to resubmit our study protocols to the FDA and IRBs for reexamination, which may impact the costs, timing or successful completion of that study. If we experience delays in completion of, or if we, the FDA or other regulatory authorities, the IRB, or other reviewing entities, or any of our clinical study sites suspend or terminate any of our clinical studies of Resunab, its commercial prospects may be materially harmed and our ability to generate product revenues will be delayed. Any delays in completing our clinical trials will increase our costs, slow down our development and approval process and jeopardize our ability to commence product sales and generate revenues. Any of these occurrences may harm our business, financial condition and prospects significantly. In addition, many of the factors that cause, or lead to, termination or suspension of, or a delay in the commencement or completion of, clinical studies may also ultimately lead to the denial of regulatory approval of Resunab. In addition, if one or more clinical studies are delayed, our competitors may be able to bring products to market before we do, and the commercial viability of Resunab could be significantly reduced.
Clinical drug development involves a lengthy and expensive process with an uncertain outcome, and results of earlier studies and trials may not be predictive of future trial results.
Clinical testing is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process. The results of pre-clinical studies and early clinical trials may not be predictive of the results of later-stage clinical trials. We cannot assure you that the FDA will view the results as we do or that any future trials of Resunab will achieve positive results. Product candidates in later stages of clinical trials may fail to show the desired safety and efficacy traits despite having progressed through pre-clinical studies and initial clinical trials. A number of companies in the biopharmaceutical industry have suffered significant setbacks in advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier trials. Any future clinical trial results for Resunab may not be successful.
In addition, a number of factors could contribute to a lack of favorable safety and efficacy results for Resunab. For example, such trials could result in increased variability due to varying site characteristics, such as local standards of care, differences in evaluation period and surgical technique, and due to varying patient characteristics including demographic factors and health status.
We intend to seek orphan drug status for Resunab for the treatment of cystic fibrosis and diffuse scleroderma, which, if approved by the FDA, will provide us with seven years of market exclusivity in the United States under the Orphan Drug Act. However, there is no guarantee that the FDA will grant any future application for orphan drug designation for Resunab, which would make us ineligible for the additional exclusivity and other benefits of orphan drug designation.
Under the Orphan Drug Act, the FDA may grant orphan drug designation to a drug intended to treat a rare disease or condition, which is generally a disease or condition that affects fewer than 200,000 individuals in the United States and for which there is no reasonable expectation that the cost of developing and making a drug available in the Unites States for this type of disease or condition will be recovered from sales of the product. Orphan drug designation must be requested before submitting an NDA. After the FDA grants orphan drug designation, the identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA. Orphan product designation does not convey any advantage in or shorten the duration of regulatory review and approval process. In addition to the potential period of exclusivity, orphan designation makes a company eligible for grant funding of up to $400,000 per year for four years to defray costs of clinical trial expenses, tax credits for clinical research expenses and potential exemption from the FDA application user fee.
If a product that has orphan designation subsequently receives the first FDA approval for the disease or condition for which it has such designation, the product is entitled to orphan drug exclusivity, which means the FDA may not approve any other applications to market the same drug for the same indication for seven years, except in limited circumstances, such as (i) the drugs orphan designation is revoked; (ii) its marketing approval is withdrawn; (iii) the orphan exclusivity holder consents to the approval of another applicants product; (iv) the orphan exclusivity holder is unable to assure the availability of a sufficient quantity of drug; or (v) a showing of clinical superiority to the product with orphan exclusivity by a competitor product. If a drug designated as an orphan product receives marketing approval for an indication broader than what is designated, it may not be entitled to orphan drug exclusivity. There can be no assurance that we will receive orphan drug designation for Resunab in the indications of cystic fibrosis, scleroderma, or other inflammatory diseases, if we elect to seek such applications.
20
Table of Contents
Third-party coverage and reimbursement and health care cost containment initiatives and treatment guidelines may constrain our future revenues.
Our ability to successfully market Resunab will depend in part on the level of reimbursement that government health administration authorities, private health coverage insurers and other organizations provide for the cost of our products and related treatments. Countries in which Resunab is expected to be sold through reimbursement schemes under national health insurance programs frequently require that manufacturers and sellers of pharmaceutical products obtain governmental approval of initial prices and any subsequent price increases. In certain countries, including the United States, government-funded and private medical care plans can exert significant indirect pressure on prices. We may not be able to sell Resunab profitably if adequate prices are not approved or coverage and reimbursement is unavailable or limited in scope. Increasingly, third-party payors attempt to contain health care costs in ways that are likely to impact our development of products including:
| | failing to approve or challenging the prices charged for health care products; |
| | introducing reimportation schemes from lower priced jurisdictions; |
| | limiting both coverage and the amount of reimbursement for new therapeutic products; |
| | denying or limiting coverage for products that are approved by the regulatory agencies but are considered to be experimental or investigational by third-party payors; and |
| | refusing to provide coverage when an approved product is used in a way that has not received regulatory marketing approval. |
Risks Relating to Our Intellectual Property Rights
It is difficult and costly to protect our intellectual property rights, and we cannot ensure the protection of these rights.
Our commercial success will depend, in part, on obtaining and maintaining patent protection for our technologies, products and processes, successfully defending these patents against third-party challenges and successfully enforcing these patents against third party competitors. The patent positions of pharmaceutical companies can be highly uncertain and involve complex legal, scientific and factual questions for which important legal principles remain unresolved. Changes in either the patent laws or in interpretations of patent laws may diminish the value of our intellectual property. Accordingly, we cannot predict the breadth of claims that may be allowable or enforceable in our patents (including patents owned by us). We currently have one issued patent and the three pending patent applications for Resunab may never be approved by United States or foreign patent offices and the existing patent and patent applications relating to Resunab and related technologies may be challenged, invalidated or circumvented by third parties and might not protect us against competitors with similar products or technologies.
The degree of future protection for our proprietary rights is uncertain, because legal means afford only limited protection and may not adequately protect our rights, permit us to gain or keep our competitive advantage, or provide us with any competitive advantage at all. For example, others have filed, and in the future are likely to file, patent applications covering products and technologies that are similar, identical or competitive to Resunab, or important to our business. We cannot be certain that any patent application owned by a third party will not have priority over patent applications filed by us, or that we will not be involved in interference, opposition or invalidity proceedings before United States or foreign patent offices.
We also rely on trade secrets to protect technology, especially in cases when we believe patent protection is not appropriate or obtainable. However, trade secrets are difficult to protect. While we require employees, academic collaborators, consultants and other contractors to enter into confidentiality agreements, we may not be able to adequately protect our trade secrets or other proprietary or licensed information. Typically, research collaborators and scientific advisors have rights to publish data and information in which we may have rights. If we cannot maintain the confidentiality of our proprietary technology and other confidential information, our ability to receive patent protection and our ability to protect valuable information owned by us may be imperiled. Enforcing a claim that a third-party entity illegally obtained and is using any of our trade secrets is expensive and time consuming, and the outcome is unpredictable. In addition, courts are sometimes less willing to protect trade secrets than patents. Moreover, our competitors may independently develop equivalent knowledge, methods and know-how.
If we fail to obtain or maintain patent protection or trade secret protection for Resunab or our technologies, third parties could use our proprietary information, which could impair our ability to compete in the market and adversely affect our ability to generate revenues and attain profitability.
We may also rely on the trademarks we may develop to distinguish our products from the products of our competitors. We cannot guarantee that any trademark applications filed by us or our business partners will be approved. Third parties may also oppose such trademark applications, or otherwise challenge our use of the trademarks. In the event that the trademarks we use are successfully challenged, we could be forced to rebrand our products, which could result in loss of brand recognition, and could require us to devote resources to advertising and marketing new brands. Further, we cannot provide assurance that competitors will not infringe the trademarks we use, or that we will have adequate resources to enforce these trademarks.
21
Table of Contents
Resunab may infringe the intellectual property rights of others, which could increase our costs and delay or prevent our development and commercialization efforts.
Our success depends in part on avoiding infringement of the proprietary technologies of others. The pharmaceutical industry has been characterized by frequent litigation regarding patent and other intellectual property rights. Identification of third party patent rights that may be relevant to our proprietary technology is difficult because patent searching is imperfect due to differences in terminology among patents, incomplete databases and the difficulty in assessing the meaning of patent claims. Additionally, because patent applications are maintained in secrecy until the application is published, we may be unaware of third-party, patents that may be infringed by commercialization of Resunab or any future product candidate. There may be certain issued patents and patent applications claiming subject matter that we may be required to license in order to research, develop or commercialize Resunab, and we do not know if such patents and patent applications would be available to license on commercially reasonable terms, or at all. Any claims of patent infringement asserted by third parties would be time-consuming and may:
| | result in costly litigation; |
| | divert the time and attention of our technical personnel and management; |
| | prevent us from commercializing a product until the asserted patent expires or is held finally invalid or not infringed in a court of law; |
| | require us to cease or modify our use of the technology and/or develop non-infringing technology; or |
| | require us to enter into royalty or licensing agreements. |
Although no third party has asserted a claim of infringement against us, others may hold proprietary rights that could prevent Resunab from being marketed. Any patent-related legal action against us claiming damages and seeking to enjoin commercial activities relating to Resunab or our processes could subject us to potential liability for damages and require us to obtain a license to continue to manufacture or market Resunab or any future product candidates. We cannot predict whether we would prevail in any such actions or that any license required under any of these patents would be made available on commercially acceptable terms, if at all. In addition, we cannot be sure that we could redesign Resunab or any future product candidates or processes to avoid infringement, if necessary. Accordingly, an adverse determination in a judicial or administrative proceeding, or the failure to obtain necessary licenses, could prevent us from developing and commercializing Resunab or a future product candidate, which could harm our business, financial condition and operating results.
A number of companies, including several major pharmaceutical companies, have conducted research on anti-inflammatory and anti-fibrosis therapies which resulted in the filing of many patent applications related to this research. If we were to challenge the validity of these or any issued United States patent in court, we would need to overcome a statutory presumption of validity that attaches to every issued United States patent. This means that, in order to prevail, we would have to present clear and convincing evidence as to the invalidity of the patents claims. If we were to challenge the validity of these or any issued United States patent in an administrative trial before the Patent Trial and Appeal Board in the United States Patent and Trademark Office, we would have to prove that the claims are unpatentable by a preponderance of the evidence. There is no assurance that a jury and/or court would find in our favor on questions of infringement, validity or enforceability.
We may be subject to claims that we have wrongfully hired an employee from a competitor or that we or our employees have wrongfully used or disclosed alleged confidential information or trade secrets of their former employers.
As is commonplace in our industry, we employ individuals who were previously employed at other pharmaceutical companies, including our competitors or potential competitors. Although no claims against us are currently pending, we may be subject in the future to claims that our employees or prospective employees are subject to a continuing obligation to their former employers (such as non-competition or non-solicitation obligations) or claims that our employees or we have inadvertently or otherwise used or disclosed trade secrets or other proprietary information of their former employers. Litigation may be necessary to defend against these claims. Even if we are successful in defending against these claims, litigation could result in substantial costs and be a distraction to management.
General Company-Related Risks
We will need to grow the size of our organization, and we may experience difficulties in managing this growth.
We currently have six employees. As our development and commercialization plans and strategies develop, we will need to expand the size of our employee base for managerial, operational, sales, marketing, financial and other resources. Future growth would impose significant added responsibilities on members of management, including the need to identify, recruit, maintain, motivate and integrate
22
Table of Contents
additional employees. In addition, our management may have to divert a disproportionate amount of its attention away from our day-to-day activities and devote a substantial amount of time to managing these growth activities. Our future financial performance and our ability to commercialize Resunab and any other future product candidates and our ability to compete effectively will depend, in part, on our ability to effectively manage our future growth.
Future capital raises may dilute our existing stockholders ownership and/or have other adverse effects on our operations.
If we raise additional capital by issuing equity securities, our existing stockholders percentage ownership will be reduced and these stockholders may experience substantial dilution. We may also issue equity securities that provide for rights, preferences and privileges senior to those of our common stock. If we raise additional funds by issuing debt securities, these debt securities would have rights senior to those of our common stock and the terms of the debt securities issued could impose significant restrictions on our operations, including liens on our assets. If we raise additional funds through collaborations and licensing arrangements, we may be required to relinquish some rights to our technologies or candidate products, or to grant licenses on terms that are not favorable to us.
If we are not successful in attracting and retaining highly qualified personnel, we may not be able to successfully implement our business strategy. In addition, the loss of the services of certain key employees, including Yuval Cohen, our CEO, Mark Tepper, our President and Chief Scientific Officer, Barbara White, our Chief Medical Officer and Sean Moran, our Chief Financial Officer would adversely impact our business prospects.
Our ability to compete in the highly competitive pharmaceuticals industry depends in large part upon our ability to attract highly qualified managerial, scientific and medical personnel. In order to induce valuable employees to remain with us, we intend to provide employees with stock options that vest over time. The value to employees of stock options that vest over time will be significantly affected by movements in our stock price that we will not be able to control and may at any time be insufficient to counteract more lucrative offers from other companies.
Our management team has expertise in many different aspects of drug development and commercialization. However, we will need to hire additional personnel as we further develop Resunab. Competition for skilled personnel in our market is intense and competition for experienced scientists may limit our ability to hire and retain highly qualified personnel on acceptable terms. Despite our efforts to retain valuable employees, members of our management, scientific and medical teams may terminate their employment with us on short notice. In connection with the Merger, we will enter into employment agreements with certain of our executive officers. However, these employment arrangements will provide for at-will employment, which means that any of our employees could leave our employment at any time, with or without notice. The loss of the services of any of our executive officers or other key employees could potentially harm our business, operating results or financial condition. In particular, we believe that the loss of the services of Yuval Cohen Ph.D., our Chief Executive Officer, Mark Tepper Ph.D., our President and Chief Scientific Officer, Barbara White, M.D., our Chief Medical Officer and Sean Moran, C.P.A., M.B.A., our Chief Financial Officer, would have a material adverse effect on our business. Our success also depends on our ability to continue to attract, retain and motivate highly skilled junior, mid-level, and senior managers as well as junior, mid-level, and senior scientific and medical personnel.
Other pharmaceutical companies with which we compete for qualified personnel have greater financial and other resources, different risk profiles, and a longer history in the industry than we do. They also may provide more diverse opportunities and better chances for career advancement. Some of these characteristics may be more appealing to high-quality candidates than what we have to offer. If we are unable to continue to attract and retain high-quality personnel, the rate and success at which we can develop and commercialize product candidates would be limited.
If product liability lawsuits are brought against us, we may incur substantial liabilities and may be required to limit commercialization of Resunab.
We face a potential risk of product liability as a result of the clinical testing of Resunab and will face an even greater risk if we commercialize Resunab or any other future product. For example, we may be sued if any product we develop, including Resunab, or any materials that we use in our products allegedly causes injury or is found to be otherwise unsuitable during product testing, manufacturing, marketing or sale. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product, negligence, strict liability and a breach of warranties. Claims could also be asserted under state consumer protection acts. If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit commercialization of Resunab. Even successful defense would require significant financial and management resources. Regardless of the merits or eventual outcome, liability claims may result in:
| | decreased demand for Resunab or any future products that we may develop; |
| | injury to our reputation; |
23
Table of Contents
| | withdrawal of clinical trial participants; |
| | costs to defend the related litigation; |
| | a diversion of managements time and our resources; |
| | substantial monetary awards to trial participants or patients; |
| | product recalls, withdrawals or labeling, marketing or promotional restrictions; |
| | the inability to commercialize Resunab; and |
| | a decline in the value of our stock. |
Our inability to obtain and retain sufficient product liability insurance at an acceptable cost to protect against potential product liability claims could prevent or inhibit the commercialization of products we develop. We intend to obtain product liability insurance covering our clinical trials. Although we will maintain such insurance, any claim that may be brought against us could result in a court judgment or settlement in an amount that is not covered, in whole or in part, by our insurance or that is in excess of the limits of our insurance coverage. Our insurance policies also have various exclusions, and we may be subject to a product liability claim for which we have no coverage. We may have to pay any amounts awarded by a court or negotiated in a settlement that exceed our coverage limitations or that are not covered by our insurance, and we may not have, or be able to obtain, sufficient capital to pay such amounts.
We may acquire businesses or products, or form strategic alliances, in the future, and we may not realize the benefits of such acquisitions.
We may acquire additional businesses or products, form strategic alliances or create joint ventures with third parties that we believe will complement or augment our existing business. If we acquire businesses with promising markets or technologies, we may not be able to realize the benefit of acquiring such businesses if we are unable to successfully integrate them with our existing operations and company culture. We may encounter numerous difficulties in developing, manufacturing and marketing any new products resulting from a strategic alliance or acquisition that delay or prevent us from realizing their expected benefits or enhancing our business. We cannot assure you that, following any such acquisition, we will achieve the expected synergies to justify the transaction.
Risks Related to our Common Stock
Our majority stockholders will control our company for the foreseeable future, including the outcome of matters requiring stockholder approval.
Our officers, directors, and five percent stockholders collectively own approximately 54.97% of our outstanding shares of common stock. In addition, these stockholders entered into a voting agreement in connection with the Merger, whereby they agreed to vote in favor of nominees for directors selected by the parties to the voting agreement as described herein. As a result, such entities and individuals will have the ability, acting together, to control the election of our directors and the outcome of corporate actions requiring stockholder approval, such as: (i) a merger or a sale of our company, (ii) a sale of all or substantially all of our assets, and (iii) amendments to our articles of incorporation and bylaws. This concentration of voting power and control could have a significant effect in delaying, deferring or preventing an action that might otherwise be beneficial to our other stockholders and be disadvantageous to our stockholders (including investors in this Offering) with interests different from those entities and individuals. Certain of these individuals also have significant control over our business, policies and affairs as officers or directors of our company. Therefore, you should not invest in reliance on your ability to have any control over our company.
An investment in our company should be considered illiquid.
An investment in our company requires a long-term commitment, with no certainty of return. Because we became a reporting company other than by the traditional means of conducting an initial public offering of our common stock, we may be unable to establish a liquid market for our common stock. In addition, investment banks may be less likely to agree to underwrite primary or secondary offerings on behalf of our company or its stockholders in the future than they would if we had become a public reporting company by means of an initial public offering of common stock. If all or any of the foregoing risks occur, it would have a material adverse effect on our company.
An active, liquid trading market for our common stock may not develop or be sustained.
Presently, our common stock is traded on the Over-the-Counter Markets, or OTC.QB, and we are in our early stages, an investment in our company will require a long-term commitment, with no certainty of return. Presently there is limited trading in our stock and in the absence of an active trading market:
24
Table of Contents
| | investors may have difficulty buying and selling or obtaining market quotations; |
| | market visibility for shares of our common stock may be limited; and |
| | a lack of visibility for shares of our common stock may have a depressive effect on the market price for shares of our common stock. |
The lack of an active market impairs your ability to sell your shares at the time you wish to sell them or at a price that you consider reasonable. The lack of an active market may also reduce the fair market value of your shares. An inactive market may also impair our ability to raise capital to continue to fund operations by selling shares and may impair our ability to acquire additional intellectual property assets by using our shares as consideration.
Even if an active trading market for our common stock develops, the market price of our common stock may be significantly volatile.
Even if an active market for our common stock develops, of which no assurances can be given, the market price for our common stock may be volatile and subject to wide fluctuations in response to factors including the following:
| | actual or anticipated fluctuations in our quarterly or annual operating results; |
| | changes in financial or operational estimates or projections; |
| | conditions in markets generally |
| | changes in the economic performance or market valuations of companies similar to ours; and |
| | general economic or political conditions in the United States or elsewhere. |
In particular, the market prices of biotechnology companies like ours have been highly volatile due to factors, including, but not limited to:
| | any delay or failure to conduct a clinical trial for our product or receive approval from the FDA and other regulatory agents; |
| | developments or disputes concerning our products intellectual property rights; |
| | our or our competitors technological innovations; |
| | changes in market valuations of similar companies; |
| | announcements by us or our competitors of significant contracts, acquisitions, strategic partnerships, joint ventures, capital commitments, new technologies, or patents; and |
| | failure to complete significant transactions or collaborate with vendors in manufacturing our product. |
The securities market has from time to time experienced significant price and volume fluctuations that are not related to the operating performance of particular companies. These market fluctuations may also materially and adversely affect the market price of shares of our common stock.
Our common stock is considered a penny stock, and is subject to additional sale and trading regulations that may make it more difficult to sell.
The Securities and Exchange Commission, or SEC, has adopted rules that regulate broker-dealer practices in connection with transactions in penny stocks. Penny stocks are generally equity securities with a price of less than $5.00 (other than securities registered on certain national securities exchanges or authorized for quotation on certain automated quotation systems, provided that current price and volume information with respect to transactions in such securities is provided by the exchange or system). The OTC.QB does not meet such requirements and if the price of our common stock is less than $5.00, our common stock will be deemed penny stock. The penny stock rules require a broker-dealer, prior to a transaction in a penny stock not otherwise exempt from those rules, to deliver a standardized risk disclosure document containing specified information. In addition, the penny stock rules require that prior to effecting any transaction in a penny stock not otherwise exempt from those rules, a broker-dealer must make a special written determination that the penny stock is a suitable investment for the purchaser and receive (i) the purchasers written acknowledgment of the receipt of a risk disclosure statement; (ii) a written agreement to transactions involving penny stocks; and (iii) a signed and dated copy of a written suitability statement. These disclosure requirements may have the effect of reducing the trading activity in the secondary market for our common stock, and therefore stock holders may have difficulty selling their shares once our common stock is publicly traded.
25
Table of Contents
FINRA sales practice requirements may also limit your ability to buy and sell our common stock, which could depress the price of our shares.
FINRA rules require broker-dealers to have reasonable grounds for believing that an investment is suitable for a customer before recommending that investment to the customer. Prior to recommending speculative low-priced securities to their non-institutional customers, broker-dealers must make reasonable efforts to obtain information about the customers financial status, tax status and investment objectives, among other things. Under interpretations of these rules, FINRA believes that there is a high probability such speculative low-priced securities will not be suitable for at least some customers. Thus, FINRA requirements make it more difficult for broker-dealers to recommend that their customers buy our common stock, which may limit your ability to buy and sell our shares once publicly traded, have an adverse effect on the market for our shares, and thereby depress our share price.
You may face significant restrictions on the resale of your shares due to state blue sky laws.
Each state has its own securities laws, often called blue sky laws, which (1) limit sales of securities to a states residents unless the securities are registered in that state or qualify for an exemption from registration, and (2) govern the reporting requirements for broker-dealers doing business directly or indirectly in the state. Before a security is sold in a state, there must be a registration in place to cover the transaction, or it must be exempt from registration. The applicable broker-dealer must also be registered in that state.
We do not know whether our securities will be registered or exempt from registration under the laws of any state. A determination regarding registration will be made by those broker-dealers, if any, who agree to serve as market makers for our common stock. We have not yet applied to have our securities registered in any state and will not do so until we receive expressions of interest from investors resident in specific states in the future. There may be significant state blue sky law restrictions on the ability of investors to sell, and on purchasers to buy, our securities. You should therefore consider the resale market for our common stock to be limited, as you may be unable to resell your shares without the significant expense of state registration or qualification.
Future sales of shares by existing stockholders could cause our stock price to decline.
As of December 31, 2014, we had outstanding options to purchase an aggregate of 3,556,691 shares of our common stock at a weighted average exercise price of $0.83 per share and warrants to purchase an aggregate of 13,709,977 shares of our common stock at a weighted average exercise price of $0.99 per share. The exercise of such outstanding options and warrants will result in further dilution of your investment. If our existing stockholders sell substantial amounts of our common stock in the public market, or if the public perceives that such sales could occur, this could have an adverse impact on the market price of our common stock, even if there is no relationship between such sales and the performance of our business.
We are an emerging growth company, and will be able take advantage of reduced disclosure requirements applicable to emerging growth companies, which could make our common stock less attractive to investors.
We are an emerging growth company, as defined in the Jumpstart Our Business Startups Act of 2012, or JOBS Act, and, for as long as we continue to be an emerging growth company, we intend to take advantage of certain exemptions from various reporting requirements applicable to other public companies but not to emerging growth companies, including, but not limited to, not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act, reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements, and exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and stockholder approval of any golden parachute payments not previously approved. We could be an emerging growth company for up to five years, or until the earliest of (i) the last day of the first fiscal year in which our annual gross revenues exceed $1 billion, (ii) the date that we become a large accelerated filer as defined in Rule 12b-2 under the Securities Exchange Act, of 1934, as amended, or the Exchange Act, which would occur if the market value of our common stock that is held by non-affiliates exceeds $700 million as of the last business day of our most recently completed second fiscal quarter, or (iii) the date on which we have issued more than $1 billion in non-convertible debt during the preceding three year period.
We intend to take advantage of these reporting exemptions described above until we are no longer an emerging growth company. Under the JOBS Act, emerging growth companies can also delay adopting new or revised accounting standards until such time as those standards apply to private companies. We have irrevocably elected not to avail ourselves of this exemption from new or revised accounting standards and, therefore, we will be subject to the same new or revised accounting standards as other public companies that are not emerging growth companies.
We cannot predict if investors will find our common stock less attractive if we choose to rely on these exemptions. If some investors find our common stock less attractive as a result of any choices to reduce future disclosure, there may be a less active trading market for our common stock and our stock price may be more volatile.
26
Table of Contents
We will incur significantly increased costs and devote substantial management time as a result of operating as a public company particularly after we are no longer an emerging growth company.
As a public company, we incur significant legal, accounting and other expenses that we did not incur as a private company. For example, we are required to comply with certain of the requirements of the Sarbanes-Oxley Act and the Dodd-Frank Wall Street Reform and Consumer Protection Act, as well as rules and regulations subsequently implemented by the SEC, including the establishment and maintenance of effective disclosure and financial controls and changes in corporate governance practices. We expect that compliance with these requirements will increase our legal and financial compliance costs and will make some activities more time consuming and costly. In addition, we expect that our management and other personnel will need to divert attention from operational and other business matters to devote substantial time to these public company requirements. In particular, we expect to incur significant expenses and devote substantial management effort toward ensuring compliance with the requirements of Section 404 of the Sarbanes-Oxley Act. In addition, after we are no longer qualify as an emerging growth company, we expect to incur additional management time and cost to comply with the more stringent reporting requirements applicable to companies that are deemed accelerated filers or large accelerated filers, including complying with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act. We are just beginning the process of compiling the system and processing documentation needed to comply with such requirements. We may not be able to complete our evaluation, testing and any required remediation in a timely fashion. In that regard, we currently do not have an internal audit function, and we will need to hire or contract for additional accounting and financial staff with appropriate public company experience and technical accounting knowledge.
We cannot predict or estimate the amount of additional costs we may incur as a result of becoming a public company or the timing of such costs.
There may be limitations on the effectiveness of our internal controls, and a failure of our control systems to prevent error or fraud may materially harm our company.
Proper systems of internal controls over financial accounting and disclosure are critical to the operation of a public company. As we are a start-up company, we only have six full time employees which results in a lack of segregation of duties and are at the very early stages of establishing, and we may be unable to effectively establish such systems, especially in light of the fact that we expect to operate as a publicly reporting company. This would leave us without the ability to reliably assimilate and compile financial information about our company and significantly impair our ability to prevent error and detect fraud, all of which would have a negative impact on our company from many perspectives.
Moreover, we do not expect that disclosure controls or internal control over financial reporting, even if established, will prevent all error and all fraud. A control system, no matter how well designed and operated, can provide only reasonable, not absolute, assurance that the control systems objectives will be met. Further, the design of a control system must reflect the fact that there are resource constraints and the benefits of controls must be considered relative to their costs. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of fraud, if any, have been detected. Failure of our control systems to prevent error or fraud could materially adversely impact us.
We may be unable to complete our analysis of our internal controls over financial reporting in a timely manner, or these internal controls may not be determined to be effective, which may adversely affect investor confidence in our company and, as a result, the value of our common stock.
We may be required, pursuant to Section 404 of the Sarbanes-Oxley Act, to furnish a report by our management on, among other things, the effectiveness of our internal control over financial reporting for the first fiscal year beginning after the effective date of a Registration Statement filed on Form S-1. This assessment will need to include disclosure of any material weaknesses identified by our management in our internal control over financial reporting, as well as a statement that our independent registered public accounting firm has issued an opinion on our internal control over financial reporting.
We are in the very early stages of the costly and challenging process of compiling the system and processing documentation necessary to perform the evaluation needed to comply with Section 404. We may not be able to complete our evaluation, testing and any required remediation in a timely fashion. During the evaluation and testing process, if we identify one or more material weaknesses in our internal control over financial reporting, we will be unable to assert that our internal controls are effective.
If we are unable to assert that our internal control over financial reporting is effective, or, if applicable, our independent registered public accounting firm is unable to express an opinion on the effectiveness of our internal controls, we could lose investor confidence in the accuracy and completeness of our financial reports, which would cause the price of our common stock to decline, and we may be subject to investigation or sanctions by the SEC. We will also be required to disclose changes made in our internal control and procedures on a quarterly basis.
27
Table of Contents
However, our independent registered public accounting firm will not be required to formally attest to the effectiveness of our internal control over financial reporting pursuant to Section 404 until the later of the year following our first annual report required to be filed with the SEC, or the date we are no longer an emerging growth company as defined in the recently enacted JOBS Act, if we take advantage (as we expect to do) of the exemptions contained in the JOBS Act. We will remain an emerging growth company for up to five years, although if the market value of our common stock that is held by non-affiliates exceeds $700 million as of any June 30th before that time, we would cease to be an emerging growth company as of the following December 31st.
At such time, our independent registered public accounting firm may issue a report that is adverse in the event it is not satisfied with the level at which our controls are documented, designed or operating. Our remediation efforts may not enable us to avoid a material weakness in our internal control over financial reporting in the future. Any of the foregoing occurrences, should they come to pass, could negatively impact the public perception of our company, which could have a negative impact on our stock price.
We do not currently intend to pay dividends on our common stock in the foreseeable future, and consequently, your ability to achieve a return on your investment will depend on appreciation in the price of our common stock.
We have never declared or paid cash dividends on our common stock and do not anticipate paying any cash dividends to holders of our common stock in the foreseeable future. Consequently, investors must rely on sales of their common stock after price appreciation, which may never occur, as the only way to realize any future gains on their investments. There is no guarantee that shares of our common stock will appreciate in value or even maintain the price at which our investors have purchased their shares.
Upon dissolution of our company, you may not recoup all or any portion of your investment.
In the event of a liquidation, dissolution or winding-up of our company, whether voluntary or involuntary, the proceeds and/or assets of our company remaining after giving effect to such transaction, and the payment of all of our debts and liabilities and distributions required to be made to holders of any outstanding preferred stock will then be distributed to the stockholders of common stock on a pro rata basis. There can be no assurance that we will have available assets to pay to the holders of common stock, or any amounts, upon such a liquidation, dissolution or winding-up of our Company. In this event, you could lose some or all of your investment.
Our ability to use our net operating loss carryforwards and certain other tax attributes may be limited.
As a result of our merger in April 2014 with Corbus Pharmaceuticals, Inc., our wholly-owned subsidiary, our ability to utilize our federal net operating loss, carryforwards and federal tax credit may be limited under Sections 382 of the Internal Revenue Code. The limitations apply if an ownership change, as defined by Section 382, occurs. Generally, an ownership change occurs if the percentage of the value of the stock that is owned by one or more direct or indirect five percent shareholders increases by more than 50 percentage points over their lowest ownership percentage at any time during the applicable testing period (typically three years). In addition, future changes in our stock ownership, which may be outside of our control, may trigger an ownership change and, consequently, Section 382 limitations. As a result, if we earn net taxable income, our ability to use our pre-change net operating loss carryforwards and other tax attributes to offset United States federal taxable income may be subject to limitations, which could potentially result in increased future tax liability to us.
Our certificate of incorporation allows for our board to create new series of preferred stock without further approval by our stockholders, which could adversely affect the rights of the holders of our common stock.
Our board of directors has the authority to fix and determine the relative rights and preferences of preferred stock. We anticipate that our board of directors will have the authority to issue up to 10,000,000 shares of our preferred stock without further stockholder approval. As a result, our board of directors could authorize the issuance of a series of preferred stock that would grant to holders the preferred right to our assets upon liquidation and the right to receive dividend payments before dividends are distributed to the holders of common stock. In addition, our board of directors could authorize the issuance of a series of preferred stock that has greater voting power than our common stock or that is convertible into our common stock, which could decrease the relative voting power of our common stock or result in dilution to our existing stockholders.
Risks Related to a Reverse Stock Split
On September 23, 2014, our board approved a reverse stock split within a range of 1:1.25 to 1:5 (the reverse stock split range), which was subsequently approved by our stockholders on October 8, 2014. If we effect a reverse stock split within the reverse stock split range, the reverse stock split may not result in a proportionate increase in the price of our common stock, in which case we may not be able to satisfy the listing requirements to support our application to be listed on NASDAQ or NYSE MKT.
Our board of directors approved a reverse stock split within a range of 1:1.25 to 1:5, or the reverse stock split range, which was subsequently approved by our stockholders on October 8, 2014. Our board of directors may effect a reverse stock split within the reverse stock split range in the event our board of directors determines that such reverse stock split is in the best interest of our stockholders and us. While
28
Table of Contents
our board of directors has not determined to effect a reverse stock split, it may determine that effecting a reverse stock split is necessary in connection with our ability to satisfy the initial listing requirements to support our application to be listed on NASDAQ or the NYSE MKT. However, the effect of a reverse stock split upon the market price of our common stock cannot be predicted with certainty, and the results of reverse stock splits by companies in similar circumstances have been varied. It is possible that the market price of our common stock following such a reverse stock split will not increase sufficiently for us to be in compliance with the minimum bid price requirement. If we are unable meet the minimum bid price requirement, we may be unable to list our shares on NASDAQ or NYSE MKT.
In the event our board of directors effects a reverse stock split within the reverse stock split range, the proposed reverse stock split may decrease the liquidity of the shares of our common stock.
In the event our board of directors effects a reverse stock split within the reverse stock split range, the liquidity of the shares of our common stock may be affected adversely by the proposed reverse stock split given the reduced number of shares that will be outstanding following the proposed reverse stock split, especially if the market price of our common stock does not increase as a result of the proposed reverse stock split. In addition, the proposed reverse stock split may increase the number of stockholders who own odd lots (less than 100 shares) of our common stock, creating the potential for such stockholders to experience an increase in the cost of selling their shares and greater difficulty effecting such sales.
In the event our board of directors effects a reverse stock split within the reverse stock split range, following such proposed reverse stock split, the resulting market price of our common stock may not attract new investors, including institutional investors, and may not satisfy the investing requirements of those investors. Consequently, the trading liquidity of our common stock may not improve.
Although we believe that a higher market price of our common stock may help generate greater or broader investor interest, there can be no assurance that the proposed reverse stock split will result in a share price that will attract new investors, including institutional investors. In addition, there can be no assurance that the market price of our common stock will satisfy the investing requirements of those investors. As a result, the trading liquidity of our common stock may not necessarily improve.
29
Table of Contents
CAUTIONARY NOTE REGARDING FORWARD-LOOKING STATEMENTS
This prospectus and the documents incorporated by reference into it contain forward-looking statements, which include information relating to future events, future financial performance, financial projections, strategies, expectations, competitive environment and regulation. Words such as may, should, could, would, predicts, potential, continue, expects, anticipates, future, intends, plans, believes, estimates, and similar expressions, as well as statements in future tense, identify forward-looking statements. Forward-looking statements should not be read as a guarantee of future performance or results and may not be accurate indications of when such performance or results will be achieved. Forward-looking statements are based on information we have when those statements are made or managements good faith belief as of that time with respect to future events, and are subject to risks and uncertainties that could cause actual performance or results to differ materially from those expressed in or suggested by the forward-looking statements. Important factors that could cause such differences include, but are not limited to:
| | our lack of operating history; |
| | our current and future capital requirements and our ability to satisfy our capital needs; |
| | our ability to complete required clinical trials of our product and obtain approval from the FDA or other regulatory agents in different jurisdictions; |
| | our ability to maintain or protect the validity of our patents and other intellectual property; |
| | our ability to retain key executive members; |
| | our ability to internally develop new inventions and intellectual property; |
| | interpretations of current laws and the passages of future laws; |
| | acceptance of our business model by investors; |
| | the accuracy of our estimates regarding expenses and capital requirements; and |
| | our ability to adequately support growth. |
The foregoing does not represent an exhaustive list of matters that may be covered by the forward-looking statements contained herein or risk factors that we are faced with that may cause our actual results to differ from those anticipate in our forward-looking statements. Please see Risk Factors for additional risks which could adversely impact our business and financial performance.
Moreover, new risks regularly emerge and it is not possible for our management to predict or articulate all risks we face, nor can we assess the impact of all risks on our business or the extent to which any risk, or combination of risks, may cause actual results to differ from those contained in any forward-looking statements. All forward-looking statements included in this prospectus are based on information available to us on the date of this prospectus. Except to the extent required by applicable laws or rules, we undertake no obligation to publicly update or revise any forward-looking statement, whether as a result of new information, future events or otherwise. All subsequent written and oral forward-looking statements attributable to us or persons acting on our behalf are expressly qualified in their entirety by the cautionary statements contained above and throughout this prospectus.
30
Table of Contents
We will not receive any of the proceeds from the sale of the common stock by the selling stockholders named in this prospectus. All proceeds from the sale of the common stock will be paid directly to the selling stockholders.
We would, however, receive proceeds upon the exercise of the warrants held by the selling stockholders which, if such warrants are exercised in full (and assuming no cashless exercise features are utilized), would be approximately $10,544,853. Proceeds, if any, received from the exercise of such warrants will be used for working capital and general corporate purposes. No assurances can be given that any of such warrants will be exercised.
We have never paid any cash dividends on our common stock. We anticipate that we will retain funds and future earnings to support operations and to finance the growth and development of our business. Therefore, we do not expect to pay cash dividends in the foreseeable future following this offering. Any future determination to pay dividends will be at the discretion of our board of directors and will depend on our financial condition, results of operations, capital requirements and other factors that our board of directors deems relevant. In addition, the terms of any future debt or credit financings may preclude us from paying dividends.
31
Table of Contents
Overview
We are a clinical stage biopharmaceutical company, focused on the development and commercialization of novel therapeutics to treat rare, life-threating inflammatory-fibrotic diseases with clear unmet medical needs. Our product Resunab, or Resunab, is a novel oral anti-inflammatory drug that is expected to commence Phase-IIa clinical trials for the treatment of scleroderma and cystic fibrosis, or CF, during the second quarter of 2015. We submitted an IND to the FDA for Resunab with the scleroderma clinical protocol on February 5, 2015. On March 5, 2015, we received FDA authorization to initiate the scleroderma clinical trial. During the second quarter of 2015, we plan to submit to the FDA under the Resunab IND an additional clinical protocol for cystic fibrosis.
Corbus Pharmaceuticals, Inc. (formerly known as JB Therapeutics, Inc.), was incorporated on April 24, 2009 under the laws of the State of Delaware. On April 11, 2014, JB Therapeutics, Inc. completed a merger with Corbus Pharmaceuticals Holdings, Inc. and changed its name to Corbus Pharmaceuticals, Inc. Upon the consummation of the merger, Corbus Pharmaceuticals, Inc. became a wholly owned subsidiary of Corbus Pharmaceuticals Holdings, Inc., or Corbus, which continues to operate the business of Corbus Pharmaceuticals, Inc. Since our inception, we have devoted substantially all of our efforts to business planning, research and development, recruiting management and technical staff, acquiring operating assets and raising capital. Our research and development activities have included completing pre-clinical studies, the development of manufacturing methods and manufacturing of our lead drug Resunab for clinical trials and the design of clinical protocols for human clinical studies.
Inflammation is a natural defense mechanism carried out by our immune system to protect our bodies from infection and injury. However, under certain circumstances inflammation once triggered is unable to be resolved, resulting in a chronic inflammatory disease. Since each organ in the body is capable of protecting itself from infection and injury by recruiting inflammatory cells to its site, each organ has the potential to suffer from excessive inflammation leading to inflammatory diseases that may cause discomfort, pain, loss of organ function, disability or even death. There are hundreds of inflammatory diseases, many of which are chronic, life-long and incurable.
A key aspect of the bodys inflammatory response is the recruitment of inflammatory cells to the site of tissue infection/injury whereupon these cells act to destroy the infection and/or repair tissue damage. The signaling pathway that modulates the inflammatory response involves the production of bioactive lipids termed eicosanoids by the enzymes cyclooxygenase, or COX, and lysyl oxidase, or LOX, resulting in pro-inflammatory mediators as shown in the Figure 1 below. These mediators trigger the activation and maintenance of a cellular inflammatory state resulting in the further generation of pro-inflammatory mediators termed cytokines. This fundamental pathway is involved in a wide spectrum of inflammatory diseases.
While the onset of inflammation has been well understood for some time, the mechanisms that resolve inflammation have only recently been discovered. This resolution pathway involves shifting the production of pro-inflammatory eicosanoids by the COX and LOX enzymes to the production of anti-inflammatory eicosanoids. These anti-inflammatory eicosanoids act to resolve inflammation and promote tissue healing. The lack of sufficient inflammatory resolution is a key contributor to many chronic inflammatory diseases.
Resunab is a synthetic, rationally designed oral small molecule that selectively binds to CB2 receptors found on immune cells. The CB2 receptor plays a natural role in modulating and resolving inflammation by, in effect, turning inflammation off. Through activation of CB2, Resunab stimulates the production of anti-inflammatory mediators and causes a concomitant reduction in pro-inflammatory mediators and cytokines. Because it acts through this natural resolving pathway, Resunab offers a new mechanism to potentially treat a wide spectrum of chronic inflammatory diseases in which the resolution of inflammation (the off switch) fails to occur.
32
Table of Contents
Figure 3: the ON and OFF cellular inflammatory pathways
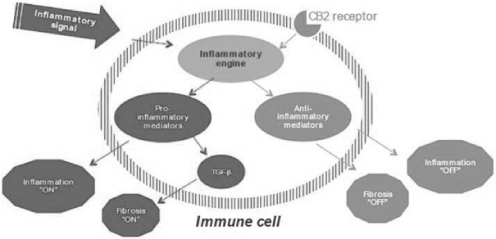
In many chronic diseases, unresolved inflammation causes progressive damage to tissues and organs resulting in excessive tissue scarring, or fibrosis, that leads to organ failure and death. Examples of such chronic diseases include cystic fibrosis, scleroderma, liver cirrhosis and non-alcoholic steatohepatitis, or NASH, chronic kidney disease, muscular dystrophies, rheumatoid arthritis, systemic lupus erythematosus and myositis. Resunab has demonstrated pre-clinical efficacy in a number of inflammatory and fibrotic disease animal models. In inflammatory models it was shown to reduce the migration of inflammatory cells into the site of inflammation, stimulate the production of the resolving (anti-inflammatory) eicosanoids, and down-regulate and reduce pro-inflammatory mediators and cytokines. In fibrosis models it was shown to reduce tissue collagen production, tissue fibrosis, stimulate the production of the resolving (anti-inflammatory) eicosanoids and reduce the pro-fibrotic cytokine TGF-beta. The net result is that Resunabthrough activation of CB2triggers a natural inflammatory resolution pathway and is therefore expected to offer a new and promising mechanism for the potential treatment of chronic inflammation and fibrosis.
Our Pipeline
The development status of Resunab is summarized below:
Figure 4: Drug developmental pipeline
33
Table of Contents
Market Opportunity in Inflammatory Diseases
The term inflammatory diseases applies to a family of diseases and conditions comprised of hundreds of distinct diseases. These include autoimmune diseases, allergies, reactions to infections and tissue breakdown, hereditary diseases as well as diseases of unknown etiology. Names of inflammatory diseases typically have the suffix its (e.g. bronchitis, appendicitis, dermatitis) but many others do not (e.g. cystic fibrosis, scleroderma, asthma, psoriasis, lupus, etc.).
While some inflammatory diseases are very common (17% of the U.S. population suffers from eczema, 10% suffers from asthma, for example), our initial focus is on a large subset of serious chronic inflammatory diseases that are rare and have no effective treatment. These diseases are categorized as orphan diseases, meaning they affect no more than 200,000 patients, each, in the U.S. Examples include cystic fibrosis, systemic scleroderma, polymyositis, dermatomyositis, primary biliary cirrhosis, pemphigus and idiopathic pulmonary fibrosis.
Markets for Resunab
Cystic Fibrosis
According to the Cystic Fibrosis Foundation, 30,000 Americans and 70,000 people worldwide suffer from CF. It is an incurable genetic pulmonary disorder characterized by the accumulation of thick, viscous secretions in the lungs. This, in turn, leads to a chronic underlying inflammation that leads to persistent bacterial infection that then causes excessive inflammation and fibrosis. Consequently, the cystic fibrosis airway is exposed to a vicious cycle of obstruction, infection, and inflammation, all intimately linked. Airway inflammation begins early in the disease course, sometimes in infants as young as four weeks old. The inflammatory process persists throughout the patients life and, if left unchecked, irreversibly damages the airways, leading to bronchiectasis and progressive decline in lung function. Gradual deterioration in breathing capacity eventually results in death with current life expectancy of approximately 40 years.
Figure 5: Factors involved in cystic fibrosis progression

Cystic fibrosis is caused by a mutation in the gene Cystic Fibrosis Transmembrane Conductance Regulator, or CFTR. The defective CFTR gene results in a chloride ion transport, leading to chronic pulmonary inflammation associated with excess mucus secretion very early in the lives of these affected patients. This chronic pulmonary inflammation damages the lung tissue and provides a fertile environment for bacteria to grow, leading to chronic bacterial infections in the lungs. This chronic infection then further exacerbates inflammation and leads to fibrosis (scarring) of the lung tissue that results in a gradual decrease in lung capacity finally resulting in death from pulmonary incapacity.
In January 2012, Vertex (Nasdaq:VRTX) launched Kalydeco, or Kalydeco, the first ever CF drug specifically targeting the underlying genetic defect in the CFTR ion channel. Kalydeco is a small synthetic oral molecule that helps correct the function of the G551D mutant CFTR protein resulting in improved breathing by approximately 10% in CF patients. However, with at least 1,300 different known mutations in the CFTR gene, Kalydeco can only be used by a specific sub-section of the CF population who suffer from a limited number of gating mutations, including the G551D mutation. Combined, these currently account for about 4.5% of the total U.S. CF patient population.
The cost of treating CF is high, with an average cost in the U.S. of $49,000 per patient per annum based on research published in 2011. Kalydeco has an annual cost of approximately $307,000 per patient, but can reach up to $370,000 for certain patients.
We believe that there is widespread agreement that a safe and effective anti-inflammatory drug that can be used chronically to treat CF patients with minimal side effects would be an invaluable addition to the therapeutic arsenal addressing this disease and should be positively received by the market.
Scleroderma
Scleroderma is a chronic connective tissue disease characterized by the thickening of the skin and is generally classified as an autoimmune rheumatic disease. According to the Scleroderma Foundation, about 300,000 Americans have scleroderma with one third having the systemic form. The disease affects mainly adults (80% of patients are women) with onset typically in the patients 30s or 40s.
34
Table of Contents
Systemic scleroderma may affect the tissues in many parts of the body. The tissues of affected organs become hard and fibrous, adversely affecting their function. There are two major recognized sub-categories of systemic scleroderma diffuse and limited with each representing about 50% of the systemic scleroderma patient population. In limited scleroderma, skin thickening is less widespread, typically confined to the fingers, hands and face, and develops slowly over years. Although internal problems occur, they are less frequent and tend to be less severe than in diffuse scleroderma, and are usually delayed in onset for several years. In diffuse scleroderma, which affects approximately 50,000 Americans, skin thickening occurs more rapidly and involves more skin areas than in limited disease and eventually can involve the skin, esophagus, gastrointestinal tract (stomach and bowels), lungs, kidneys, heart and other internal organs. Diffuse scleroderma patients have a high mortality rate with approximately 50% survival over a 10-year period.
There are currently no cures or effective therapies for diffuse scleroderma. While not fully understood, it is believed that inflammation leading to fibrosis is the driving force behind the diseases progress, symptoms and eventual mortality. In particular, the pro-fibrotic cytokine TGF beta has been identified as a key player in the progression of the disease and, we believe, is an important target for diffuse scleroderma therapy.
Current Treatment Alternatives for Inflammatory Diseases
Overview
Drugs used to treat inflammatory diseases are broadly divided into two classes: steroids and non-steroidal anti-inflammatory drugs. Non-steroidal drugs, in turn, can be categorized into synthetic drugs, which include Resunab, and biological drugs, which include monoclonal antibody and protein therapies. Synthetic drugs are typically administered orally while biologic drugs generally need to be administered by injection. According to Global Business Intelligence Research, the global market for drugs to treat inflammation in 2010 was approximately $58 billion and is expected to grow to approximately $86 billion by 2017.
Corticosteroids are the most commonly prescribed medications for treating inflammatory diseases because of their high potency, unparalleled formulation flexibility, and low cost. However, chronic corticosteroid use is limited by adverse side effects that include hypertension, high glucose levels/diabetes, obesity, brittle bones/osteoporosis, immunosuppression/increased infection, glaucoma and psychosis. Thus, safer yet potent alternatives to steroids have long been sought to fill this unmet medical need. We believe the global market for corticosteroids was approximately $88 billion in 2013.
Non-steroid anti-inflammatory synthetic drugs, or NSAIDs, include the older generation of non-specific COX inhibitors, such as ibuprofen, naproxen, and Aspirin (possibly the most commonly used drug in the world), and a newer generation of specific inhibitors of COX-2, such as Celebrex®, or Celebrex, and Vioxx. COX inhibitors are drugs that inhibit the action of the COX enzymes, which are responsible for producing factors that promote inflammation (known as pro-inflammatory eicosanoids). The older generation of COX inhibitors inhibits both COX-1 and COX-2 and is associated with severe gastrointestinal adverse effects. The newer generation of NSAID drugs which are specific for COX-2, originally designed to be safer in terms of gastrointestinal side effects, have subsequently been found to have cardiovascular side effects. These side effects have led to the withdrawal of the drug Vioxx from the market and specific black-box warnings for the related drug Celebrex. The market for oral NSAIDs was approximately $5.4 billion in 2013.
Non-steroid biological drugs are used to treat severe cases of inflammation in autoimmune diseases. These drugs are large molecule proteins produced from live cells and not by way of artificial chemical synthesis. Examples of this type of drug are Enbrel® and Remicade®, both of which are used for treating severe rheumatoid arthritis and psoriasis as well as inflammatory bowel disease. These drugs have a number of disadvantages including that the drugs must be administered by injection/IV, their costs are high and they are associated with increased incidence of malignancy and infection. This is the largest market of anti-inflammatory drugs with anti-TNF therapies for rheumatoid arthritis alone projected to reach $23 billion by 2015, according to Global Industry Analysts.
Cystic Fibrosis
The importance of inflammation (both underlying and infection-driven) in CF treatment is universally accepted, but we believe current anti-inflammatory treatments present a paradox: while treatment with systemic steroid and ibuprofen (a COX 1 & 2 inhibitor) are clearly effective in improving the symptoms of CF, the side effects associated with chronic treatment using these drugs are significant and as a result these drugs have limited long-term utility. Specifically, long term usage of oral corticosteroids in children gives rise to such side effects as glucose intolerance, cataract formation, multiple bone fractures secondary to osteoporosis or osteopenia, Cushing Syndrome effects, and anorexia nervosa as well as growth retardation. The side effects of high doses of ibuprofen taken for an extended duration are mainly gastrointestinal side effects. Other therapies routinely used by CF patients include antibiotics, such as Cayston from Gilead, and TOBI from Novartis, and mucolytics, such as Pulmozyme from Genentech. In addition, Vertex currently markets the only approved drug, Kalydeco, specifically targeting the defective protein product of the CFTR gene mutation in CF. However, with at least 1,300 known mutations in the CFTR gene, Kalydeco can only be used by a specific sub-section of the CF patient population who suffer from a limited number of gating mutations including the G551D mutation. Combined, these currently account for about 4.5% of the total U.S. CF patient population.
35
Table of Contents
Diffuse Scleroderma
Current medications for scleroderma focus on treating the four main features of the disease: inflammation, autoimmunity, vascular disease, and tissue fibrosis. For inflammation, the most commonly prescribed medicines for scleroderma are NSAIDs and corticosteroids. As described above, these medicines have significant adverse effects when given chronically, but more important they have not proven to be effective in treating scleroderma. For autoimmunity, the most commonly prescribed medicines for scleroderma are immunosuppressants. These include methotrexate, cyclosporine, anti-thymocyte globulin, mycophenolate mofetil, azathioprine, and cyclophosphamide. While these have been shown to have some benefit, they are effective only in a limited number of cases and have serious side effects including increased infection and malignancy. For vascular disease, the most commonly prescribed medicines for scleroderma are medicines which improve blood flow to target organs affected by the disease and reduce blood pressure. These include calcium channel blockers, angiotensin converting enzyme, or ACE inhibitors, endothelin-1 receptor inhibitors and prostacyclins. While these drugs are effective for the treatment of some of the vascular complications of scleroderma they have no benefit for the inflammatory or fibrotic manifestations. The last class of drugs for the treatment of scleroderma is the anti-fibrotics. The most commonly prescribed anti-fibrotic medicines for scleroderma are colchicine, para-aminobenzoic acid, or PABA, dimethyl sulfoxide, and D-penicillamine. These drugs are typically of limited benefit and are used fairly infrequently. Recently the drug pirfenidone was approved in Europe and the United States for the treatment of Idiopathic Pulmonary Fibrosis (a disease that also causes fibrosis of the lungs). However, its effectiveness in treating scleroderma has not been established.
Resunabs Mechanism of Action is Distinct from NSAIDs and Steroids
Corticosteroids and NSAIDs exert their effect by inhibiting inflammation. In simple terms, both classes of drugs inhibit inflammation by interfering with the biochemical pathways in the cell that promote and sustain inflammation. For example, NSAID directly inhibit the activity of the COX 1 and COX 2 enzymes that are responsible for generating pro-inflammatory eicosanoids. A drawback of this approach is that it only inhibits one arm of the eicosanoid pathway (e.g. COX but not LOX) resulting in an increase in LOX-derived inflammatory mediators which leads to gastrointestinal and cardiovascular side effects (termed molecular shunting).
Resunab, on the other hand, activates the natural pathways that resolve inflammation, the so called resolving pathway or off-switch. By doing so, we believe that Resunab is less likely to cause the side effects that result from the accumulation of certain pro-inflammatory eicosanoids. We also believe Resunabs unique mechanism of action is expected to provide a safer and potentially more effective treatment for chronic inflammation than the current alternatives- steroids and NSAIDs. Resunab may have the potential to safely treat a wide spectrum of chronic inflammatory diseases in which the resolution of inflammation, or the off switch, fails to occur.
Safety & Toxicology
To date, Resunab has undergone an extensive battery of animal safety and toxicology studies in support of Phase II clinical development. Unlike other CB2 agonists, Resunab exhibits limited blood brain barrier penetration and negligible CB1 activity in vivo resulting in limited central nervous system side effects. Results of the safety pharmacology studies in animals assessing the central nervous system, cardiovascular and respiratory systems, renal system and gastrointestinal system were all negative and support that there should be a significant safety margin at anticipated therapeutics doses of Resunab in patients.
Animal toxicological profiles of orally administered Resunab in single and multi-dose studies in mice, rats, and dogs, and a battery of in vitro and in vivo genetic toxicity studies, have been conducted, including a chronic rat toxicology that was requested by the FDA and successfully completed. The results of these studies showed no major toxicological concerns and an excellent safety margin based on drug exposure levels in animals compared to human exposure. In support of Phase II clinical trials, thirteen-week GLP toxicology studies have been completed in rats and dogs. Based on the results of these studies and prior clinical trials, the safety margin in humans is estimated to be between 8 and 32 times greater than the doses planned for our next clinical trials.
Pre-clinical Results
In pre-clinical studies, Resunab has demonstrated clear efficacy at resolving inflammation in a number of animal pharmacology models in which inflammation was induced by a variety of means: arachidonic acid, Zymosin, PAF, IL-1-beta, TNF-alpha and Freunds complete adjuvant. Similarly, fibrosis was induced in skin tissue by bleomycin and TGF beta receptor activation and in lung tissue by bleomycin. Of particular note, Resunab suppressed tissue destruction in several of these disease models. At the cellular level, in various models Resunab acted to reduce the migration of inflammatory cells into the site of inflammation, stimulate the production of the resolving mediators LXA4 and PGJ2, and down regulate and reduce the pro-inflammatory cytokines (IL-1ß and IL-6) and the pro-fibrotic cytokine TOF-beta.
Effect of Resunab in Fibrotic Disease Animal Models
The efficacy of Resunab was investigated in three mouse models of scleroderma. Oral administration of Resunab once-a-day at 1 mg/kg/day inhibited dermal fibrosis in the three models as measured by reductions in dermal thickness, markers of collagen production, and
36
Table of Contents
myofibroblast abundance (cells that produce collagen). Histopathologic evaluation revealed that Resunab inhibited the fibrosis of the skin tissue in each of these models. In addition, oral administration of Resunab was effective at inhibiting lung fibrosis in a bleomycin-induced mouse scleroderma model. Collectively, we believe this data supports the development of Resunab as a potent and novel anti-fibrotic/anti-inflammatory drug with the potential to treat some of the key manifestations of human scleroderma.
Figure 6: Resunab inhibition of skin thickening in Mouse Scleroderma Model
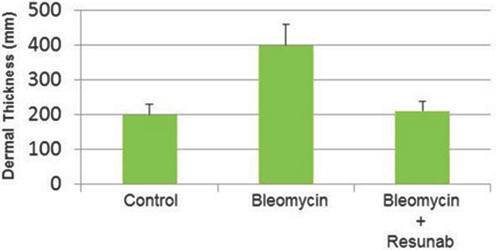
To translate these in vivo effects of Resunab on fibrosis in animal models to humans, we determined the anti-fibrotic effects of Resunab on dermal fibroblasts isolated from diffuse cutaneous scleroderma patients. Dermal fibroblasts from scleroderma patients overproduce extracellular matrix proteins like collagen and the pro-fibrotic cytokine TGF-beta. Further supporting its anti-fibrotic activity, Resunab inhibited new collagen synthesis, reduced TGF-beta and increased anti-inflammatory (resolving) eicosanoid levels in this ex-vivo model of human scleroderma. These responses were statistically significant with a p<0.001 as determined using the Student-Newmen Keuls post-hoc test for multiple comparisons. TGF-beta has been identified in published scientific literature to be an important cytokine in promoting inflammation and fibrosis in multiple diseases and conditions including scleroderma and cystic fibrosis. While no pre-clinical model is 100% predictive of clinical efficacy, the results from our pre-clinical data provide a rationale for further clinical development.
Human Clinical Results to Date
Two Phase I and one Phase IIa clinical trials have been conducted by prior licensees Atlantic Pharmaceuticals and Indevus Pharmaceuticals, Inc. who were developing Resunab as an analgesia therapy (pain relief) rather than an anti-inflammatory therapy. Based on their review of the preclinical and clinical data in pain relief, Indevus Pharmaceuticals elected not to continue with further clinical trials and its license rights were terminated in December 2008. Upon termination, the rights reverted back to Dr. Sumner Burstein who then assigned the rights to us in April 2009.
The first Phase I study evaluated the safety, tolerability and pharmacokinetics of a single oral dose of Resunab in healthy adult male subjects over a dose range from 1 mg to 10 mg, in 4 dose groups of 8 subjects each. Resunab had satisfactory oral bioavailability, was well tolerated, and exhibited linear pharmacokinetics over the dose range tested. There were no life-threatening or serious adverse events in this study. Two subjects in the 3 mg group and one subject in the 6 mg group out of a total of twenty-four subjects reported adverse events of mild to moderate intensity. None of the remaining subjects in the 3 mg and 6 mg groups and no subjects in the 1 mg, 10 mg and placebo groups experienced any adverse events. The two subjects in the 3 mg group reported blurred vision, difficulty in remembering, mild euphoria, impression of slower movements, dry mouth and difficulty in concentrating. The one subject in the 6 mg group reported orthostatic vagal fainting, feeling dizzy, and nausea immediately after the first blood draw, which occurred prior to the administration of the drug.
The second Phase I study evaluated the safety, tolerability and pharmacokinetics of single and multiple ascending doses of Resunab at higher doses. Each dose level had 8 subjects randomized at a ratio of 6 receiving Resunab and 2 receiving placebo. Doses ranged from 10 to 240 mg single dose, and 20, 40 and 80 mg three times a day, or tid, for 7 days multi-dose. Resunab showed good tolerability at single doses up to 120 mg and multiple doses up to 40 mg three times a day for 7 days. For the single dose treatment stage, the most frequently occurring
37
Table of Contents
treatmentemergent adverse events, or TEAEs, occurring in > 10% of all subjects treated with Resunab, in decreasing order of frequency, were: dizziness (15 out of 48), nausea (10 out of 48), vomiting (7 out of 48), pallor (6 out of 48), dry mouth (5 out of 48), headache (5 out of 48), somnolence (5 out of 48), tremor (5 out of 48), and disorientation (5 out of 48). All TEAEs were mild to moderate with the majority of these events occurred in subjects treated at dose levels of 120 mg and above. For the multiple dose stage, there were no TEAEs at 20 mg tid while in the 40 and 80 mg tid dose groups the most frequently occurring TEAEs, occurring in > 10% of all subjects treated with Resunab, were at the 40 and 80 mg tid dose respectively: dizziness (4 out of 6 and 3 out of 6), nausea (2 out of 6 and 1 out of 6), somnolence (2 out of 6 and 1 out of 6), dry mouth (1 out of 6 and 1 out of 6), fatigue (0 out of 6 and 2 out of 6), feeling abnormal (0 out of 6 and 2 out of 6), anorexia (0 out of 6 and 2 out of 6), inappropriate affect (0 out of 6 and 2 out of 6), and orthostatic hypotension (0 out of 6 and 2 out of 6). The majority of these events were mild and occurred in subjects treated at the highest dose level of approximately 80 mg three times a day, for 7 days (i.e., subjects treated with 80 mg tid were reduced to 60 mg tid starting with the second dose on Day 2 continuing through Day 7). In some elderly patients over 65 years of age, changes in electrocardiogram readings were noted; however no differences in readings were observed between subjects treated with Resunab versus and placebo thus this was not deemed to be of clinical relevance. Resunab exhibited linear pharmacokinetics over the dose range tested.
A Phase IIa crossover design study was conducted for Resunab in refractory neuropathic pain patients, or NP. In this study, 21 NP patients were treated with either Resunab or placebo at a dose of 20 and 40 mg twice a day (8 hours apart) for 1 week followed by a 1 week washout and a cross over. Resunab reduced the 3 hour pain index by up to 28% (p<0.03) in one cohort, and was effective at reducing pain by >30% in 50% of this same cohort (P<0.03) of refractory pain patients although its analgesic effect wore off between 3-8 hours post-dose. Resunab was well tolerated and there were no safety issues of note in this study.
While Resunab showed a clear analgesic signal in this phase IIa study in refractory neuropathic pain patients, we are not relying on these efficacy results to support our clinical program as this study was designed to measure pain while our future studies will have a completely different efficacy endpoint.
Clinical Development Plan
Overview
Our clinical development plan for Resunab is to conduct two independent multicenter Phase IIa randomized, double-blind, placebo-controlled, three-arm clinical trials of three month treatment duration to evaluate the safety, efficacy and pharmacokinetics of Resunab in patients with cystic fibrosis and diffuse scleroderma. We believe that upon obtaining adequate safety and proof of concept efficacy data, the next step following our planned Phase IIa studies, would be to conduct a pivotal multi-center Phase II/III clinical trial in each indication with the objective of establishing the dose-effect relationship and optimal dose of Resunab. These studies will be designed with input from regulatory authorities with the aim of gaining expedited development and review by the United States Food and Drug Administration, or FDA, through the following FDA programs: Fast Track designation; Accelerated Approval, and Priority Review designation. These FDA expedited programs for serious conditions are designed to facilitate the development and expedite the review of new drugs that are intended to treat serious or life-threatening conditions and that demonstrate the potential to address unmet medical needs. We must request Fast Track designation from the FDA. The request can be initiated at any time during the drug development process. FDA will review the request and make a decision within 60 days based on whether the drug fulfills an unmet medical need in a serious condition. A drug that receives Fast Track designation is eligible for some or all of the following: (i) more frequent meetings with FDA to discuss the drugs development plan and ensure collection of appropriate data needed to support drug approval; (ii) more frequent written correspondence from FDA about things such as the design of the proposed clinical trial and the use of biomarkers; and (iii) eligibility for Accelerated Approval and Priority Review, if relevant criteria are met. Under its accelerated approval authority, FDA may approve a product for a serious or life threatening disease or condition, including a fast track product, if it is found to have an effect on a surrogate endpoint that is reasonably likely to predict a clinical benefit. FDA may also approve a product under accelerated approval authority if it is found to have an effect on a clinical endpoint that can be measured earlier than an effect on irreversible morbidity or mortality (also referred to as an intermediate endpoint). The evidence to support accelerated approval may be epidemiological, pathophysiological, therapeutic, and pharmacologic or based on the use of biomarkers. Accelerated Approval can be withdrawn or the labeled indication of the drug changed if trials fail to verify clinical benefit or do not demonstrate sufficient clinical benefit to justify the risk associated with the drug. Every drug application submitted to the FDA is subject to consideration for Priority Review designation, even if the applicant does not request it. FDA informs the applicant of a Priority Review Designation within 60 days of the receipt of the original New Drug Application, or NDA. Designation of a drug as Priority does not alter the scientific/medical standard for approval or the quality of evidence necessary for approval. Priority review shortens the time period for review of an NDA (6 months compared with the 10 month standard review). There is no guarantee that we will receive Fast Track designation, Accelerated Approval designation, or Priority Review designation for any of our product candidates, and even if we do receive such designation, that our NDA will be approved.
38
Table of Contents
Scleroderma
On February 5, 2015, we submitted an IND to the FDA for Resunab with the clinical protocol for a Phase IIa double-blind placebo controlled clinical study evaluating Resunab in patients with diffuse scleroderma at three dosing levels, 5 mg and 20 mg once-a-day and 20 mg twice a day, versus placebo. On March 5, 2015, we received FDA authorization to initiate the scleroderma clinical trial and we expect to initiate the trial during the second quarter of 2015. The trial design will have a four-week screening period, 12-week treatment period and a four-week safety follow-up. The study planned is a U.S. multi-center trial. The lead Principal Investigator will be Dr. Robert Spiera of the Hospital of Special Surgery, New York City, New York. Patients will be screened and those meeting trial criteria will be randomized to one of four arms. Patients will be monitored for safety and tolerability throughout the study. The primary goal of this trial is to establish safety of Resunab in diffuse scleroderma patients and efficacy based on a change in the Combined Response Index in diffuse cutaneous Systemic Sclerosis. Secondary endpoint measurements will include patient assessment scores, drug action biomarkers, disease biomarkers and metabolipidomic profiles.
Cystic Fibrosis
During the second quarter of 2015, we plan to submit an additional clinical protocol under the Resunab IND for a Phase IIa double-blind placebo controlled study evaluating Resunab in CF at initial dosing levels for the first month of 1mg and 5mg per day and then 20 mg once a day and 20 mg twice a day, versus placebo. We expect to initiate the clinical study during the second quarter of 2015. Patients in the study will be 18-30 years of age with mild to moderate cystic fibrosis as assessed by lung function tests. The trial design will have a two-week screening period, followed by a 12-week active treatment period, and then a four-week safety follow-up. The study planned is a multi-center U.S. and European trial. The lead Principal Investigators in the U.S. will be Dr. James Chmiel of the Rainbow Babies & Childrens Hospital, Cleveland, Ohio and in the E.U., Dr. Stuart Elborn of Queens University Hospital, Belfast, Ireland. Patients will be screened and those meeting the trial criteria will be randomized into one of four arms. Patients will be monitored for safety and tolerability throughout the study. The primary goal of this trial is to establish safety of Resunab in CF patients and an efficacy assessment based on pulmonary function and the reduction of inflammatory markers. Secondary efficacy assessments will include the CF biomarker score, patient scores and drug action biomarkers.
Competition
There are numerous drug therapies currently used to treat CF patients, but, to our knowledge, none have been developed specifically to address the inflammatory aspect of the disease. Antibiotics address the pulmonary bacterial infection and mucolytics address the accumulation of mucus in the lungs. The average CF patient uses all of these therapies since they each address a different aspect of the disease. Anti-inflammatories, oral corticosteroids and very high doses of ibuprofen, are used intermittently with some clinical benefit, but, due to their adverse side effects are not used chronically.
Vertex currently markets the only approved drug, Kalydeco, specifically targeting the defective protein product of the CFTR gene mutation in CF. However, it is only effective for approximately 8% of the total U.S. CF patient population that have one of ten specific CFTR gene mutations. Kalydeco was approved by the FDA January 2012 and has an average annual cost of $307,000 per year per patient. N30 is a private company developing a nitric oxide modulator that is in a Phase II study for broncheodilatory and anti-inflammatory activity.
Unlike cystic fibrosis, there are no approved drugs for the specific treatment of scleroderma. Nonetheless, physicians do treat scleroderma patients with a number of drugs including immunosupressants and cytotoxics to try to reduce the autoimmune response of the disease. However, these drugs have not proven to be very effective in treating scleroderma and there remains a high unmet need for new effective drugs to treat the progressive fibrosis in scleroderma. Because of this several companies, including Bristol Myers Squibb Company (NYSE: BMY), Promedior, Sanofi (NYSE: SNY), Digna Biotech, FibroGen, Inc. (Nasdaq: FGEN) and Biogen Idec, Inc. (Nasdaq: BIIB), are actively working to developing new drugs for scleroderma which target inflammation and/or fibrosis. To the best of our knowledge, Resunab offers a unique mode of action to treat scleroderma being one of the few oral drugs having both anti-inflammatory and anti-fibrotic properties.
Research and Development
We incurred approximately $1,256,000 and $211,000 for research and development activities for the years ended December 31, 2014 and 2013, respectively. These expenses include cash and non-cash expenses relating to the development of our clinical and pre-clinical programs for Resunab. Prior to the Corbus formation, Resunab was licensed to several other companies which conducted extensive pre-clinical and clinical development work on the drug, including development of a manufacturing process, pre-clinical safety, toxicology and pharmacology studies, two Phase I clinical trials and a Phase II clinical trial in neuropathic pain.
Intellectual Property
Our intellectual property and product pipeline is based on seminal research done by Professor Sumner Burstein, Ph.D. at the University of Massachusetts Medical Center and patents filed by Corbus directly. Upon Corbus formation, Dr. Burstein assigned to Corbus his
39
Table of Contents
rights and intellectual property ownership to Resunab on a royalty-free basis in consideration for 200,000 shares of Series A Non-Convertible preferred stock. The intellectual property includes scientific data and regulatory data, product know-how and one patent issued in January 2014 and expiring in November 2029 for the use of Resunab to treat interstitial cystitis, an indication for which we are currently pursuing partnership opportunities.
Since acquiring the asset, we have filed three new patent applications for Resunab, which if granted, would extend intellectual property protection through at least 2033. The three new patent filings cover:
| | A composition of matter claim based on an improved ultrapure version of Resunab; |
| | Resunabs use in treating a number of pulmonary fibrotic diseases including cystic fibrosis, scleroderma and IPFr fibrosis; and |
| | Specific Resunabs dosing regimens and formulations. |
We also plan to request the FDA and other worldwide regulatory agencies to grant orphan drug status for Resunab for the treatment of scleroderma, cystic fibrosis and possibly other orphan inflammatory diseases. While there can be no assurance that such status will be granted, prior FDA actions indicate that this is likely. Orphan drug status provides seven years of market exclusivity in the U.S. and ten years in Europe beginning on the date of drug approval.
Our commercial success depends in part on our ability to obtain and maintain patent and other proprietary protection for Resunab and to operate without infringing the proprietary right of others and to prevent others from infringing our proprietary rights. We strive to protect our intellectual property through a combination of patents, and trademarks as well as through the confidentiality provisions in our contracts. With respect to Resunab, we endeavor to obtain and maintain patent protection in the United States and internationally on all patentable aspects of the drug. We cannot be sure that the patents will be granted with respect to any patent applications we may own or license in the future, nor can we be sure that our existing patents or any patents we may own or license in the future will be useful in protecting our technology. For this and more comprehensive risks related to our intellectual property, please see Risk FactorsRisks Relating to Our Intellectual Property Rights.
In addition to patents, we rely on trade secrets and know-how to develop and maintain our competitive position. For example, significant aspects of our proprietary technology platform are based on unpatented trade secrets and know-how. Trade secrets and know-how can be difficult to protect. We seek to protect our proprietary technology and processes, in part, by confidentiality agreements and invention assignment agreements with our employees, consultants, scientific advisors, contractors and commercial partners. These agreements are designed to protect our proprietary information and, in the case of the invention assignment agreements, to grant us ownership of technologies that are developed through a relationship with a third party. We also seek to preserve the integrity and confidentiality of our data and trade secrets by maintaining physical security of our premises and physical and electronic security of our information technology systems. While we have confidence in these individuals, organizations and systems, agreements or security measures may be breached, and we may not have adequate remedies for any breach. In addition, our trade secrets may otherwise become known or be independently discovered by competitors. To the extent that our contractors use intellectual property owned by others in their work for us, disputes may arise as to the rights in related or resulting know-how and inventions.
We also plan to seek trademark protection in the United States and outside of the United States where available and when appropriate. We intend to use these registered marks in connection with our pharmaceutical research and development as well as our product candidates.
Manufacturing and Supply for Resunab
We have developed and validated a good manufacturing practice, or GMP, process to manufacture Resunab through our contract manufacturer. This contract manufacturer has already produced multi-Kg scale bulk batches of the active pharmaceutical ingredient under GMP for our Phase II clinical studies and is capable of producing sufficient active ingredient for all the clinical studies required prior to submitting an NDA to the FDA. We do not own or operate manufacturing facilities for the production of Resunab. We expect to depend on third-party suppliers and manufacturing organizations for all of our clinical trial quantities of raw materials and drug substance. Resunab is a synthetic molecule and there are readily available supplies of all raw materials needed for the manufacture of Resunab.
Regulatory Matters
Government Regulation
Any product development activities related to Resunab or products that we may develop or acquire in the future will be subject to extensive regulation by various government authorities, including the FDA and other federal, state and local statutes and regulations and comparable regulatory authorities in other countries, which regulate the design, research, clinical and non-clinical development, testing, manufacturing, storage, distribution, import, export, labeling, advertising and marketing of pharmaceutical products and devices. Generally, before a new drug can be sold, considerable data demonstrating its quality, safety and efficacy must be obtained, organized into a format
40
Table of Contents
specific to each regulatory authority, submitted for review and approved by the regulatory authority. The data is often generated in two distinct development states: pre-clinical and clinical. Resunab or other products that we may develop or acquire in the future must be approved by the FDA through the IND process before they may be legally marketed in the United States. For new chemical entities, the pre-clinical development stage generally involves synthesizing the active component, developing the formulation and determining the manufacturing process, as well as carrying out non-human toxicology, pharmacology and drug metabolism studies which support subsequent clinical testing.
The clinical stage of development can generally be divided into three sequential phases that may overlap, Phase I, Phase II and Phase III clinical trials. In Phase I, generally, small numbers of healthy volunteers are initially exposed to single escalating doses and then multiple escalating doses of the product candidate. The primary purpose of these studies is to assess the metabolism, pharmacologic action, side effect tolerability and safety of the drug. Phase II trials typically involve studies in disease-affected patients to determine the dose required to produce the desired benefits, while Phase IIb trials are designed to determine efficacy. At the same time, safety and further pharmacokinetic and pharmacodynamic information is collected. In some instances, formal Phase I and Phase II trials may not be deemed necessary or required by the FDA. Such is often the case when the safety and efficacy of an active ingredient is considered to be well understood by the FDA. Under established regulatory frameworks, pharmaceutical products with active ingredients equal or similar to those known by the FDA often enter more streamlined development programs than compounds entirely new to the agency.
Post-approval studies, sometimes referred to as Phase IV clinical trials, may be conducted after initial marketing approval. Sometimes, these studies are used to gain additional experience from the treatment of patients in the intended therapeutic condition, then often referred to as Phase IV clinical trials. In certain instances, the FDA may mandate the performance of Phase IV studies. In other situations, post-approval studies aim to gain additional indications for a medication, then often indicated as Phase IIIb studies.
Development of Drugs in the United States
In the United States, the process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local and foreign statutes and regulations require the expenditure of substantial time and financial resources. Failure to comply with the applicable United States requirements at any time during the product development process, approval process or after approval, may subject an applicant to administrative or judicial sanctions. These sanctions could include the FDAs refusal to approve pending applications, withdrawal of an approval, a clinical hold, warning letters, product recalls or withdrawals from the market, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, restitution, disgorgement, or civil or criminal penalties. Any agency or judicial enforcement action could have a material adverse effect on us.
Prior to the start of human clinical studies for a new drug in the United States, pre-clinical laboratory and animal tests are often performed under the FDAs Good Laboratory Practices regulations. The sponsor must submit the result of the pre-clinical tests, together with manufacturing information, analytical data and any available clinical data or literature and a proposed clinical protocol to the FDA as part of an IND application, which is a request for authorization from the FDA to administer an investigational drug or biological product to humans. Similar filings are required in other countries. The amount of data that must be supplied in the IND depends on the phase of the study. Phase I studies typically require less data than larger Phase II and III studies. A clinical plan must be submitted to the FDA prior to commencement of a clinical trial. If the FDA has concerns about the clinical plan or the safety of the proposed studies, they may suspend or terminate the study at any time. Studies must be conducted in accordance with good clinical practice and regulator reporting of study progress and any adverse experiences is required. Studies are also subject to review by independent institutional review boards responsible for overseeing studies at particular sites and protecting human research study subjects. An independent institutional review board may also suspend or terminate a study once initiated. Accordingly, we cannot be sure that submission of an IND will result in the FDA allowing clinical trials to begin, or that once begun, issues will not arise that could cause the trial to be suspended or terminated.
Review and Approval in the United States
Following pivotal or Phase III trial completion, data is analyzed to determine safety and efficacy. Data is then filed with the FDA in a New Drug Application, or an NDA, along with proposed labeling for the product and information about the manufacturing and testing processes and facilities that will be used to ensure product quality. In the United States, FDA approval of an NDA must be obtained before marketing a pharmaceutical product. The NDA must contain proof of safety, purity, potency and efficacy, which entails extensive pre-clinical and clinical testing.
The FDA will likely re-analyze the clinical trial data, which could result in extensive discussions between the FDA and us during the review process. The review and evaluation of applications by the FDA is extensive and time consuming and may take several years to complete. The FDA may conduct a pre-approval inspection of the manufacturing facilities for the new product to determine whether they comply with current good manufacturing practice requirements and may also audit data from clinical and pre-clinical trials.
41
Table of Contents
There is no assurance that the FDA will act favorably or quickly in making such reviews and significant difficulties or costs may be encountered in our efforts to obtain FDA approvals. The FDA may require that certain contraindications, warnings or precautions be including in the product labeling, or may condition the approval of the NDA on other changes to the proposed labeling, development of adequate controls and specifications, or a commitment to conduct post-marketing testing or clinical trials and surveillance programs to monitor the safety of approved products that have been commercialized. Further, the FDA may place conditions on approvals including the requirement for a risk evaluation and mitigation strategy, or REMS, to assure the safe use of the drug. If the FDA concludes a REMS is needed, the sponsor of the NDA must submit a proposed REMS; the FDA will not approve the NDA without an approved REMS, if required. A REMS could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. Any of these limitations on approval or marketing could restrict the commercial promotion, distribution, prescription or dispensing of products. Product approvals maybe withdrawn for non-compliance with regulatory standards or if problems occur, following the initial marketing of the product.
Orphan Drug Designation
Under the Orphan Drug Act, the FDA may grant orphan drug designation to a drug intended to treat a rare disease or condition, which is generally a disease or condition that affects fewer than 200,000 individuals in the United States and for which there is no reasonable expectation that the cost of developing and making a drug available in the Unites States for this type of disease or condition will be recovered from sales of the product. Orphan product designation must be requested before submitting an NDA. After the FDA grants orphan drug designation, the identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA. Orphan product designation does not convey any advantage in or shorten the duration of regulatory review and approval process. In addition to the potential period of exclusivity, orphan designation makes a company eligible for grant funding of up to $400,000 per year for four years to defray costs of clinical trial expenses, tax credits for clinical research expenses and potential exemption from the FDA application user fee.
If a product that has orphan designation subsequently receives the first FDA approval for the disease or condition for which it has such designation, the product is entitled to orphan drug exclusivity, which means the FDA may not approve any other applications to market the same drug for the same indication for seven years, except in limited circumstances, such as (i) the drugs orphan designation is revoked; (ii) its marketing approval is withdrawn; (iii) the orphan exclusivity holder consents to the approval of another applicants product; (iv) the orphan exclusivity holder is unable to assure the availability of a sufficient quantity of drug; or (v) a showing of clinical superiority to the product with orphan exclusivity by a competitor product. If a drug designated as an orphan product receives marketing approval for an indication broader than what is designated, it may not be entitled to orphan drug exclusivity. There can be no assurance that we will receive orphan drug designation for Resunab in the indications of cystic fibrosis, scleroderma, or other orphan inflammatory diseases.
Drug Development in Europe
In the European Union, our future products may also be subject to extensive regulatory requirements. Similar to the United States, the marketing of medicinal products has been subject to the granting of marketing authorizations by regulatory agencies. Particular emphasis is also being placed on more sophisticated and faster procedures for reporting of adverse events to the competent authorities.
As in the United States, the various phases of pre-clinical and clinical research in the European Union are subject to significant regulatory controls. Although the regulatory controls on clinical research are currently undergoing a harmonization process following the adoption of the Clinical Trials Directive 2001/20/EC, there are currently significant variations in the member state regimes. All member states, however, currently require independent institutional review board approval of interventional clinical trials. Except for the United Kingdom Phase I studies in health volunteers, all clinical trials require either prior governmental notification or approval. Most regulators also require the submission of adverse event reports during a study and a copy of the final study report.
Review and Approval in the European Union
In the European Union, approval of new medicinal products can be obtained through one of three processes: the mutual recognition procedure, the centralized procedure and the decentralized procedure. We intend to determine which process we will follow, if any, in the future.
Mutual Recognition Procedure: An applicant submits an application in one European Union member state, known as the reference member state. Once the reference member state has granted the marketing authorization, the applicant may choose to submit applications in other concerned member states, requesting them to mutually recognize the marketing authorizations already granted. Under this mutual recognition process, authorities in other concerned member states have 55 days to raise objections, which must then be resolved by discussion among the concerned member states, the reference member state and the applicant within 90 days of the commencement of the mutual recognition procedure. If any disagreement remains, all considerations by authorities in the concerned member states are suspended and the disagreement is resolved through an arbitration process. The mutual recognition procedure results in separate national marketing authorizations in the reference member state.
42
Table of Contents
Centralized Procedure: This procedure is currently mandatory for products developed by means of a biotechnological process and optional for new active substances and other innovative medicinal products with novel characteristics. Under this procedure, an application is submitted to the European Agency for the Evaluation of Medical Products. Two European Union member states are appointed to conduct an initial evaluation of each application. These countries each prepare an assessment report that is then used as the basis of a scientific opinion of the Committee on Proprietary Medical Products. If this opinion is favorable, it is sent to the European Commission, which drafts a decision. After consulting with the member states, the European Commission adopts a decision and grants a marketing authorization, which is valid throughout the European Union and confers the same rights and obligations in each of the member states as a marketing authorization granted by that member state.
Decentralized Procedure: The most recently introduced of the three processes for obtaining approval of new medicinal processes in the European Union, the decentralized procedure is similar to the mutual recognition procedure described above, but with differences in the timing that key documents are provided to concerned member states by the reference member state, the overall timing of the procedure and the possibility of, among other things, clock stops during the procedure.
Post-Marketing Requirements
Following approval of a new product, a pharmaceutical company and the approved product are subject to continuing regulation by the FDA and other federal and state regulatory authorities, including, among other things, monitoring and recordkeeping activities, reporting to applicable regulatory authorities of adverse experiences with the product, providing the regulatory authorities with updated safety and efficacy information, product sampling and distribution requirements, and complying with promotion and advertising requirements, which include, among others, standards for direct-to-consumer advertising, restrictions on promoting drugs for uses or in patient populations not described in the drugs approved labeling (known as off-label use), limitations on industry-sponsored scientific and educational activities, and requirements for promotional activities involving the internet. Although physicians may prescribe legally available drugs for off-label uses, manufacturers may not market or promote such off-label uses. Modifications or enhancements to the products or labeling or changes of site of manufacture are often subject to the approval of the FDA and other regulators, which may or may not be received or may result in a lengthy review process.
Prescription drug advertising is subject to federal, state and foreign regulations. In the United States, the FDA regulates prescription drug promotion, including direct-to-consumer advertising. Prescription drug promotion materials must be submitted to the FDA in conjunction with their first use. Any distribution of prescription drug products and pharmaceutical samples must comply with the U.S. Prescription Drug Marketing Act, a part of the U.S. Federal Food, Drug and Cosmetic Act. Once a product is approved, its manufacture is subject to comprehensive and continuing regulations by the FDA. The FDA regulations require the products be manufactured in specific approved facilities and in accordance with current good manufacturing practices, and NDA holders must list their products and register their manufacturing establishments with the FDA. These regulations also impose certain organizational, procedural and documentation requirements with respect to manufacturing and quality assurance activities. Drug manufacturers and other entities involved in the manufacture and distribution of approved drugs are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with current good manufacturing practice and other laws. NDA holders using contract manufacturers, laboratories or packagers are responsible for the selection and monitoring of qualified firms. These firms are subject to inspections by the FDA at any time, and the discovery of violative conditions could result in enforcement actions that interrupt the operation of any such facilities or the ability to distribute products manufactured, processed or tested by them.
Special Protocol Assessment
The Federal Food, Drug and Cosmetic Act directs the FDA to meet with sponsors, pursuant to a sponsors written request, for the purpose of reaching agreement on the design and size of clinical trials intended to form the primary basis of an efficacy claim in an NDA. If an agreement is reached, the FDA will reduce the agreement to writing and make it part of the administrative record. This agreement is called a special protocol assessment, or SPA. While the FDAs guidance on SPAs states that documented SPAs should be considered binding on the review division, the FDA has latitude to change its assessment if certain exceptions apply. Exceptions include public health concerns emerging that were unrecognized at the time of the protocol assessment, identification of a substantial scientific issue essential to the safety or efficacy testing that later comes to light, a sponsors failure to follow the protocol agreed upon, or the FDAs reliance on data, assumptions or information that are determined to be wrong.
Other Regulatory Matters
Manufacturing, sales, promotion and other activities following product approval are also subject to regulation by numerous regulatory authorities in addition to the FDA, including, in the United States, the Centers for Medicare & Medicaid Services, or CMS, other divisions of the Department of Health and Human Services, the Drug Enforcement Administration, the Consumer Product Safety Commission, the Federal Trade Commission, the Occupational Safety & Health Administration, the Environmental Protection Agency, and state and local governments.
43
Table of Contents
Sales, marketing and scientific/educational programs must also comply with federal and state fraud and abuse laws. Pricing and rebate programs must comply with the Medicaid rebate requirements of the U.S. Omnibus Budget Reconciliation Act of 1990. If products are made available to authorized users of the Federal Supply Schedule of the General Services Administration, additional laws and requirements apply. The handling of any controlled substances must comply with the U.S. Controlled Substances Act and Controlled Substances Import and Export Act. Products must meet applicable child-resistant packaging requirements under the U.S. Poison Prevention Packaging Act. Manufacturing, sales, promotion and other activities are also potentially subject to federal and state consumer protection and unfair completion laws.
The distribution of pharmaceutical products is subject to additional requirements and regulations, including extensive record-keeping, licensing, storage and security requirements intended to prevent the unauthorized sale of pharmaceutical products.
Third-Party Payer Coverage and Reimbursement
Significant uncertainty exists as to the coverage and reimbursement status of any of our drug candidates that ultimately may obtain regulatory approval. In both the United States and foreign markets, our ability to commercialize our product candidates successfully, and to attract commercialization partners for our product candidates, depends in significant part on the availability of adequate financial coverage and reimbursement from third-party payers, including, in the United States, governmental payers such as the Medicare and Medicaid programs, managed care organizations, and private health insurers. Medicare is a federally funded program managed by the CMS, through local fiscal intermediaries and carriers that administer coverage and reimbursement for certain healthcare items and services furnished to the elderly and disabled. Medicaid is an insurance program for certain categories of patients whose income and assets fall below state defined levels and who are otherwise uninsured that is both federally and state funded and managed by each state. The federal government sets general guidelines for Medicaid and each state creates specific regulations that govern its individual program. Each payer has its own process and standards for determining whether it will cover and reimburse a procedure or particular product. Private payers often rely on the lead of the governmental payers in rendering coverage and reimbursement determinations. Therefore, achieving favorable CMS coverage and reimbursement is usually a significant gating issue for successful introduction of a new product. The competitive position of some of our products will depend, in part, upon the extent of coverage and adequate reimbursement for such products and for the procedures in which such products are used. Prices at which we or our customers seek reimbursement for our product candidates can be subject to challenge, reduction or denial by the government and other payers.
The United States Congress and state legislatures may, from time to time, propose and adopt initiatives aimed at cost containment, which could impact our ability to sell our product candidates profitably. For example, in March 2010, President Obama signed into law the Patient Protection and Affordable Care Act and the associated reconciliation bill, which we refer to collectively as the Health Care Reform Law, a sweeping law intended to broaden access to health insurance, reduce or constrain the growth of healthcare spending, enhance remedies against fraud and abuse, add new transparency requirements for healthcare and health insurance industries, impose new taxes and fees on the health industry and impose additional health policy reforms. Effective October 1, 2010, the Health Care Reform Law revised the definition of average manufacturer price for reporting purposes, which could increase the amount of Medicaid drug rebates to states once the provision is effective. Further, the law imposes a significant annual fee on companies that manufacture or import branded prescription drug products. Substantial new provisions affecting compliance have also been enacted, which may require us to modify our business practices with healthcare practitioners. We will not know the full effects of the Health Care Reform Law until applicable federal and state agencies issue regulations or guidance under the new law. Although it is too early to determine the effect of the Health Care Reform Law, the new law appears likely to continue the pressure on pharmaceutical pricing, especially under the Medicare program, and may also increase our regulatory burdens and operating costs. Moreover, in the coming years, additional changes could be made to governmental healthcare programs that could significantly impact the success of our product candidates.
The cost of pharmaceuticals continues to generate substantial governmental and third-party payer interest. We expect that the pharmaceutical industry will experience pricing pressures due to the trend toward managed healthcare, the increasing influence of managed care organizations and additional legislative proposals. Our results of operations could be adversely affected by current and future healthcare reforms.
Some third-party payers also require pre-approval of coverage for new or innovative devices or drug therapies before they will reimburse healthcare providers that use such therapies. While we cannot predict whether any proposed cost-containment measures will be adopted or otherwise implemented in the future, the announcement or adoption of these proposals could have a material adverse effect on our ability to obtain adequate prices for our product candidates and operate profitably.
In addition, in some foreign countries, the proposed pricing for a drug must be approved before it may be lawfully marketed. The requirements governing drug pricing vary widely from country to country. For example, the European Union provides options for its member states to restrict the range of medicinal products for which their national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. A member state may approve a specific price for the medicinal product or it may instead adopt a system of direct or indirect controls on the profitability of the company placing the medicinal product on the market. There can be no assurance
44
Table of Contents
that any country that has price controls or reimbursement limitations for pharmaceutical products will allow favorable reimbursement and pricing arrangements for any of our products. Historically, products launched in the European Union do not follow price structures of the United States and generally tend to be significantly lower.
Other Healthcare Laws and Compliance Requirements
In the United States, our activities are potentially subject to regulation by various federal, state and local authorities in addition to the FDA, including the CMS, other divisions of the United States Department of Health and Human Services (e.g., the Office of Inspector General), the United States Department of Justice and individual United States Attorney offices within the Department of Justice, and state and local governments. These regulations include:
| | the federal healthcare program anti-kickback law which prohibits, among other things, persons from soliciting, receiving or providing remuneration, directly or indirectly, to induce either the referral of an individual, for an item or service or the purchasing or ordering of a good or service, for which payment may be made under federal healthcare programs such as the Medicare and Medicaid programs; |
| | federal false claims laws which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid, or other government reimbursement programs that are false or fraudulent. The government may assert that a claim including items or services resulting from a violation of the federal healthcare program anti-kickback law or related to off-label promotion constitutes a false or fraudulent claim for purposes of the federal false claims laws; |
| | the federal Health Insurance Portability and Accountability Act of 1996 which prohibits executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters and which also imposes certain requirements relating to the privacy, security and transmission of individually identifiable health information; |
| | the federal transparency requirements under the Health Care Reform Law requires manufacturers of drugs, devices, biologics, and medical supplies to report to the Department of Health and Human Services information related to physician payments and other transfers of value and physician ownership and investment interests; |
| | the Federal Physician Payments Sunshine Act within the ACA, and its implementing regulations, require that certain manufacturers of drugs, devices, biological and medical supplies for which payment is available under Medicare, Medicaid or the Childrens Health Insurance Program (with certain exceptions) to report information related to certain payments or other transfers of value made or distributed to physicians and teaching hospitals, or to entities or individuals at the request of, or designated on behalf of, the physicians and teaching hospitals and to report annually certain ownership and investment interests held by physicians and their immediate family members; and |
| | state law equivalents of each of the above federal laws, such as anti-kickback and false claims laws, which may apply to items or services reimbursed by any third party payer, including commercial insurers, and state laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and often are not preempted by federal laws, thus complicating compliance efforts. |
In addition, we may be subject to data privacy and security regulation by both the federal government and the states in which we conduct our business. The Health Insurance Portability and Accountability Act, or HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act, or HITECH, and its implementing regulations, imposes certain requirements relating to the privacy, security and transmission of individually identifiable health information. Among other things, HITECH makes HIPAAs privacy and security standards directly applicable to business associatesindependent contractors or agents of covered entities that receive or obtain protected health information in connection with providing a service on behalf of a covered entity. HITECH also created four new tiers of civil monetary penalties, amended HIPAA to make civil and criminal penalties directly applicable to business associates and possibly other persons, and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorneys fees and costs associated with pursuing federal civil actions. In addition, state laws govern the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts.
Post-Marketing Regulations
Following approval of a new product, a pharmaceutical company and the approved product are subject to continuing regulation by the FDA and other federal and state regulatory authorities, including, among other things, monitoring and recordkeeping activities, reporting to
45
Table of Contents
applicable regulatory authorities of adverse experiences with the product, providing the regulatory authorities with updated safety and efficacy information, product sampling and distribution requirements, and complying with promotion and advertising requirements, which include, among others, standards for direct-to-consumer advertising, restrictions on promoting drugs for uses or in patient populations not described in the drugs approved labeling (known as off-label use), limitations on industry-sponsored scientific and educational activities, and requirements for promotional activities involving the internet. Although physicians may prescribe legally available drugs for off-label uses, manufacturers may not market or promote such off-label uses. Modifications or enhancements to the products or labeling or changes of site of manufacture are often subject to the approval of the FDA and other regulators, which may or may not be received or may result in a lengthy review process.
Emerging Growth Company
We are an emerging growth company, as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act, and, for as long as we continue to be an emerging growth company, we may choose to take advantage of exemptions from various reporting requirements applicable to other public companies but not to emerging growth companies, including, but not limited to, not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act of 2002, reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements, and exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and stockholder approval of any golden parachute payments not previously approved. We could be an emerging growth company for up to five years, or until the earliest of (i) the last day of the first fiscal year in which our annual gross revenues exceed $1 billion, (ii) the date that we become a large accelerated filer as defined in Rule 12b-2 under the Securities Exchange Act of 1934, as amended, which would occur if the market value of our common stock that is held by non-affiliates exceeds $700 million as of the last business day of our most recently completed second fiscal quarter, or (iii) the date on which we have issued more than $1 billion in non-convertible debt during the preceding three-year period. We are choosing to opt out of the extended transition periods available under the JOBS Act for complying with new or revised accounting standards, and intend to take advantage of the other exemptions.
Employees
We have six full time employees. All of our employees are engaged in administration, finance, clinical, manufacturing, regulatory and business development functions. We believe our relations with our employees are good. We anticipate that the number of employees will grow as we continue to develop our product candidates. In addition, we utilize and will continue to utilize consultants, clinical research organizations and third parties to perform our pre-clinical studies, clinical studies, manufacturing and regulatory functions.
Facilities
Our principal offices are 100 River Ridge Drive, Norwood, MA 02062. We signed a three year lease which commenced on July 1, 2014, at an annual cost of $54,900. We believe our facilities are adequate for our foreseeable needs.
Legal Matters
We are not currently subject to any material legal proceedings. However, we may from time to time become a party to various legal proceedings arising in the ordinary course of our business.
46
Table of Contents
MANAGEMENT AND BOARD OF DIRECTORS
The following sets forth certain information with respect to our executive officers and directors.
| Name |
Age | Position(s) |
||
| Yuval Cohen, Ph.D. |
40 | Chief Executive Officer, Director | ||
| Mark Tepper, Ph.D. |
57 | President and Chief Scientific Officer | ||
| Barbara White, M.D. |
64 | Chief Medical Officer | ||
| Sean Moran |
57 | Chief Financial Officer | ||
| Alan Holmer |
65 | Director | ||
| David P. Hochman |
39 | Director | ||
| Renu Gupta |
59 | Director | ||
| Avery W. Catlin |
66 | Director | ||
Management
Yuval Cohen, Ph.D., Chief Executive Officer and Director
Dr. Cohen has served as our Chief Executive Officer and one of our directors since the Merger. Dr. Cohen joined JB Therapeutics as its Chief Executive Officer in July 2013. Prior to joining JB Therapeutics, he was the President and co-founder of Celsus Therapeutics PLC (Nasdaq CM: CLTX) from 2005 until February 2013, and as Senior Vice President from February 2013 until June 2013. Dr. Cohen was also a board member of Celsus until December 2013. Starting as a small startup with seed financing, under Dr. Cohens leadership, Celsus developed five novel anti-inflammatory drug candidates with two reaching Phase IIb stages focusing on allergies and autoimmune diseases of the skin (eczema), airways (cystic fibrosis and hay fever), digestive tract (inflammatory bowel disease) and eye (conjunctivitis). Dr. Cohen participated in all stages of the pre-clinical and clinical development from project management to interactions with regulatory bodies and with the investment community in fundraising. Apart from his industry experience, he is also the author of a number of peer-reviewed papers and reviews as well as listed inventor on a number of patents. Dr. Cohen holds a KS. in microbiology and biochemistry from University of Cape Town, South Africa, and has a Ph.D., summa cum laude, from the Curie Institute of Cancer Research in Paris and the University of Paris V.
Mark A. Tepper, Ph.D., President and Chief Scientific Officer
Dr. Tepper has served as our President and Chief Scientific Officer since the Merger. He has more than twenty five years of management experience in pharmaceutical R&D. During the last 12 years, Dr. Tepper has focused on identifying unique early stage biotechnology assets which fill a significant unmet medical need and has founded or co-founded three new biotech companies, including Corbus, to commercialize these assets. Prior to joining JB Therapeutics in January 2012, Dr. Tepper was a consultant to the biotechnology and pharmaceutical industry from 2009-2011. Prior to that he was President and Chief Executive Officer of NKT Therapeutics Inc. from 2007-2008 and before that President of RXi Pharmaceuticals from 2003 to 2007. Dr. Tepper served at EMD Serono from 1995 to 2002, most recently as Vice President of Research and Operations where he played a key role in the development and commercialization of the fertility drug Gonal-F and multiple sclerosis drug Rebif. While with Bristol Myers Squibb from 1988 to 1995, most recently as Senior Research Investigator, he was a member of the project team responsible for developing the cancer drug Taxol and the rheumatoid arthritis drug Orencia. Dr. Tepper received a Ph.D. in Biochemistry & Biophysics from Columbia University, College of Physicians & Surgeons, New York, and a B.A in Chemistry with Highest Honors from Clark University, Worcester, Massachusetts. He gained postdoctoral training at the University of Massachusetts Medical School, Worcester, Massachusetts in the laboratory of Professor Michael P. Czech.
Barbara White, M.D., Chief Medical Officer
Dr. White has served as our Chief Medical Officer since August 2014. Previously, Dr. White served as Senior Vice President and Head of Research and Development at Stiefel, a dermatological pharmaceutical division of GlaxoSmithKline, a public pharmaceutical company, from 2011 to 2013. From 2010 to 2011, Dr. White was Vice President and Head of Immunology Therapeutic Area at UCB, a public biopharmaceutical manufacturing company. At MedImmune, LLC, a subsidiary of AstraZeneca plc, a public pharmaceutical company, Dr.
47
Table of Contents
White served first as Senior Director of Clinical Development from 2006 until 2007, and then as Vice President until 2010. Prior to her pharmaceutical career, Dr. White was Professor and Associate Chair of Research, Department of Medicine, at the University of Maryland School of Medicine. She was formerly Associate Chief of Staff, Research Service, at the Baltimore Veteran Administration (VA) Medical Center, where her research focused on immune-mediated mechanisms of lung fibrosis in scleroderma. Barbara also previously served as Co-Director of the Johns Hopkins University and University of Maryland Scleroderma Center. Barbara received her medical degree from the University of Pennsylvania School of Medicine and is board certified in internal medicine, rheumatology and allergy/clinical immunology. She completed her postdoctoral studies in basic cellular immunology at the National Institutes of Health.
Sean Moran, CPA, MBA, Chief Financial Officer
Mr. Moran has served as our Chief Financial Officer since the Merger. Mr. Moran joined JB Therapeutics as its Chief Financial Officer in January 2014. Mr. Moran has twenty years of senior financial experience with emerging biotechnology, drug delivery and medical device companies. Mr. Moran has worked at three different companies that completed initial public offerings and maintained a listing on a public exchange. Before joining Corbus, Mr. Moran served as Chief Financial Officer for InVivo Therapeutics Corporation from 2010 to 2013, Celsion Corporation from 2008 to 2010, Transport Pharmaceuticals Inc. from 2006 to 2008, Echo Therapeutics Inc. from 2002 to 2006, SatCon Technology Corporation from 2000 to 2002, and Anika Therapeutics Inc. from 1993 to 2000. Mr. Moran is a CPA by training and earned his M.B.A. and a B.S. in Accounting from Babson College.
Directors
Yuval Cohen, Ph.D., Chief Executive Officer and Director
See description under Management.
Alan Holmer, Director
Mr. Holmer became a director of Corbus Pharmaceutical in January 2014 and became one of our directors in connection with the Merger. From 1996 to 2005 he served as President and Chief Executive Officer of the Pharmaceutical Research and Manufacturers of America (PhRMA), an organization that represents the worldwide interests of leading pharmaceutical and biotechnology companies, based in Washington, D.C. From 2005 to 2007 and again from February 2009 until its acquisition by Merck in May 2011, Mr. Holmer served as a Director of Inspire Pharmaceuticals, Inc., and at various times as member of its Corporate Governance Committee, Audit Committee, and Drug Development Committee. In addition to his pharmaceutical industry experience, Mr. Holmer has significant expertise in handling legal, international trade and governmental issues, having held various positions within the office of the U.S. Trade Representative, the Commerce Department and the White House, including serving as Deputy U.S. Trade Representative with rank of Ambassador. Mr. Holmer served as Special Envoy for China and the Strategic Economic Dialogue, a position to which he was appointed by Secretary of the Treasury, Henry M. Paulson, Jr. from 2007 to 2009. Mr. Holmer also served as a partner at the international law firm, Sidley & Austin (now Sidley Austin LLP), and as an associate at Steptoe & Johnson LLP. Since January 2012, Mr. Holmer has served as Special Counsel in the Washington, D.C. office of Smith, Currie & Hancock LLP. Mr. Holmer has been involved in many community service organizations, included currently serving as the Chairman of the Board of the Metropolitan Washington, D.C., Chapter of the Cystic Fibrosis Foundation. He also served as Co-Chairman of the Presidents Advisory Council on HIV/AIDS. Mr. Holmer received an A.B. degree from Princeton University and a J.D. from Georgetown University Law Center.
David P. Hochman, Director
Mr. Hochman has been one of our directors since December 2013. Since June 2006, Mr. Hochman has been Managing Partner of Orchestra Medical Ventures, LLC, an investment firm that employs an innovative strategy to create, build and invest in medical technology companies intended to generate substantial clinical value and superior investor returns. He is also President of Accelerated Technologies, Inc. (ATI), a medical device accelerator managed by Orchestra. He has over eighteen years of venture capital and investment banking experience. Mr. Hochman is the Chairman of Vital Access Corp. and MOTUS GI Medical Technologies Ltd., as well as a director of Caliber Therapeutics, BackBeat Medical , FreeHold Surgical, Maternity Neighborhood, Inc. and Naked Brand Group, Inc. (OCT.QB:NAKD). Prior to joining Orchestra, Mr. Hochman was Chief Executive Officer of Spencer Trask Edison Partners, LLC, a principal investment partnership focused on early stage healthcare companies. He was also Managing Director of Spencer Trask Ventures, Inc. during which time he was responsible for directing the firms venture banking group and led financing transactions for over twenty early-stage companies. Mr. Hochman was a board advisor of Health Dialog Services Corporation, a world leader in collaborative care management that was acquired in 2008 by the British United Provident Association for $750 million. From 2005 to 2007, he was a co-founder and director of PROLOR Biotech, Inc., a biopharmaceutical company developing longer-lasting versions of approved therapeutic proteins, which was purchased by Opko Health (NYSE: OPK) in 2013 for over $600 million. Mr. Hochman also currently serves as a board member of two non-profit organizations: the Citizens Committee for New York City and the Mollie Parnis Livingston Foundation. He graduated with honors from the University of Michigan.
Dr. Renu Gupta, Director
Dr. Gupta became one of our directors in June 2014. Dr. Gupta has more than 25 years of drug development, regulatory and senior management experience within the biopharma industry. Renu is currently special advisor to the CEO of Insmed having served as Chief Medical
48
Table of Contents
Officer there since 2008. Previously Renu has served as the Executive Vice President Development and Chief Medical Officer of Transave, Inc. since September 2006, and has been a Director of the UK subsidiary, Transave Inhalation Biotherapeutics as of May 2008. From May 2003 to August 2006, she held the position of Senior Vice President Development at Antigenics, Inc. Prior to that, she served at Novartis as Vice President and Head of U.S. Clinical Research and Development and Global Head of Cardiovascular, Metabolics, Endocrine and Gastroenterology Research. Renu also spent almost 10 years at Bristol-Myers Squibb, where she was responsible for clinical research, business development and global development and marketing strategy for infectious diseases and immunology. She received her bachelor and medical degrees from the University of Zambia and completed her medical and post-doctoral training at Albert Einstein Medical Center, the Wistar Institute of Anatomy and Biology, Childrens Hospital of Philadelphia, and the University of Pennsylvania, where she was Adjunct Assistant Professor until 1997. Her work has been published in leading peer-reviewed journals and she has been active in numerous relevant academic and professional societies. Renu is a founding member of the Industrial Management Board at the Harvard Medical School, served as Chair of the Medical Advisory Council for Antigenics, past member of the Scientific Advisory Board at Cerimon Pharmaceuticals, and the Institute of Medicine Forum on Emerging Infections, and is a Board Member of Aim at Melanoma, formerly Charlie Guild Melanoma Foundation.
Avery W. (Chip) Catlin, Director
Mr. Catlin became one of our directors in August 2014. Currently, Mr. Catlin also serves as Senior Vice President, Chief Financial Officer, and Secretary of Celldex Therapeutics, Inc., a public biopharmaceutical company. Prior to joining Celldex Therapeutics, Inc. in January 2000, he served as Vice President, Operations and Finance, and Chief Financial Officer of Endogen, Inc., a public life science research products company, from 1996 to 1999. From 1992 to 1996, he held various financial positions at Repligen Corporation, a public biopharmaceutical company, serving the last two years as Chief Financial Officer. Earlier in his career, he held the position of Chief Financial Officer at MediSense, Inc., a Massachusetts-based medical device company. Mr. Catlin received his B.A. degree from the University of Virginia and M.B.A. from Babson College and is a Certified Public Accountant.
Board Committees
Our board of directors has established an Audit Committee, a Compensation Committee and a Nominating and Corporate Governance Committee. Our board of directors may establish other committees to facilitate the management of our business. The composition and functions of each committee are described below. Members serve on these committees until their resignation or until otherwise determined by our board of directors. Each of these committees operate under a charter that has been approved by our board of directors.
Audit Committee. Our Audit Committee consists of Mr. Holmer, Dr. Gupta and Mr. Catlin and Mr. Catlin is the Chairman of the Audit Committee. Our board of directors has determined that the three directors currently serving on our Audit Committee are independent within the meaning of The NASDAQ Marketplace Rules and Rule 10A-3 under the Exchange Act. In addition, our board of directors has determined that Mr. Catlin qualifies as an audit committee financial expert within the meaning of SEC regulations and The NASDAQ Marketplace Rules.
The Audit Committee oversees and monitors our financial reporting process and internal control system, reviews and evaluates the audit performed by our registered independent public accountants and reports to the board any substantive issues found during the audit. The Audit Committee will be directly responsible for the appointment, compensation and oversight of the work of our registered independent public accountants. The Audit Committee reviews and approves all transactions with affiliated parties. The board has adopted a written charter for the Audit Committee, which is available on our website.
Compensation Committee. Our Compensation Committee consists of Mr. Holmer, Dr. Gupta and Mr. Catlin and Mr. Holmer is the Chairman of the Compensation Committee. Our board of directors has determined that the three directors currently serving on our Compensation Committee are independent under the listing standards, are non-employee directors as defined in Rule 16b-3 promulgated under the Exchange Act and are outside directors as that term is defined in Section 162(m) of the Internal Revenue Code of 1986, as amended.
The Compensation Committee provides advice and makes recommendations to the board in the areas of employee salaries, benefit programs and director compensation. The Compensation Committee also reviews and approves corporate goals and objectives relevant to the compensation of our President, Chief Executive Officer, and other officers and makes recommendations in that regard to the board as a whole. The board has adopted a written charter for the Compensation Committee, which is available on our website.
Nominating and Corporate Governance Committee. Our Nominating and Corporate Governance Committee consists of Mr. Holmer, Dr. Gupta and Mr. Catlin and Mr. Holmer is the Chairman of the Nominating and Corporate Governance Committee. The Nominating and Corporate Governance Committee nominates individuals to be elected to the full board by our stockholders. The Nominating and Corporate Governance Committee considers recommendations from stockholders if submitted in a timely manner in accordance with the procedures set forth in our Bylaws and will apply the same criteria to all persons being considered. All members of the Nominating and Corporate Governance Committee are independent directors as defined under the NASDAQ listing standards. The board has adopted a written charter for the Nominating and Corporate Governance Committee, which is available on our website.
49
Table of Contents
Director Independence
Our board of directors undertook a review of its composition, the composition of its committees and the independence of each director. Based upon information requested from and provided by each director concerning his or her background, employment and affiliations, including family relationships, our board of directors has determined that Mr. Holmer, Dr. Gupta and Mr. Catlin do not have a relationship that would interfere with the exercise of independent judgment in carrying out the responsibilities of a director and that each of these directors is independent as that term is defined under the Rules of the NASDAQ Stock Market and the SEC.
Scientific Advisory Board
We believe in seeking and attracting scientific and clinical leaders in the fields of immunology and inflammatory diseases to provide counsel and support our growth. We currently have a scientific advisory board of five members.
Sumner Burstein, Ph.D.
Dr. Burstein co-founded the Company and has been a faculty member of the Department of Biochemistry & Molecular Pharmacology at The University of Massachusetts Medical School since 1977. His research activities have centered on the structure and function of natural and synthetic cannabinoids (unrelated to cannabis) and their mechanism of action. His research led to the discovery of the principal route of metabolism of THC, from which he demonstrated that terminal carboxylic acid metabolites of THC are non-psychoactive, yet retain their activity as analgesic and anti-inflammatory agents. This resulted in the design and discovery of ajulemic acid (Resunab), which is being pursued by the Company. More recently, he discovered a new family of lipid signaling molecules called lipoamino acids. Earlier in his career, Dr. Burstein was a Senior Scientist at The Worcester Foundation for Experimental Biology where, in addition to his studies on cannabinoids, he worked in the areas of steroids and prostaglandins biochemistry. Dr. Burstein received his doctoral degree at Wayne State University, a masters degree at Brandeis University and a bachelors degree at MIT, all in the field of chemistry. He was a Postdoctoral Fellow in the department of Prof. Efraim Katchalski at The Weitzman Institute in Israel.
Ethan Burstein, Ph.D.
Ethan Burstein is Senior Director of Biosciences at ACADIA Pharmaceuticals Inc., where he leads drug discovery pharmacology and is responsible for advancement of preclinical leads into IND-track development. Dr. Burstein has published over 70 peer-reviewed papers on the molecular pharmacology of G-protein coupled receptors and discovery of small molecule receptor ligands, and is one of the inventors of ACADIAs R-SAT® high-throughput screening technology. Prior to ACADIA, Dr. Burstein was a research fellow at the University of Vermont where he received a National Research Service Award Fellowship to study the structural basis of receptor/G-protein signaling. Dr. Burstein received his PhD in Toxicology at the University of Rochester.
Robert B. Zurier, M.D.
Robert B. Zurier, M.D., has been Professor of Medicine at the University of Massachusetts Medical School in Worcester since 1991, and was Chief of Rheumatology there until 2007. From 1980 to 1991 he was Professor of Medicine and Chief of Rheumatology at the University of Pennsylvania School of Medicine in Philadelphia. Dr. Zurier graduated from the University of Texas Southwestern Medical School in Dallas, trained in Internal Medicine at Boston City Hospital, then practiced general internal medicine in Holden, Massachusetts, for three years before training in clinical and research rheumatology at NYU-Bellevue Medical Center in New York City. Dr. Zuriers clinical, research, and teaching accomplishments have been recognized by election to the American Society of Clinical Investigation and the Interurban Clinical Club (President, 1987), inclusion in Whos Who In America and Best Doctors in America, designation as Master of the American College of Rheumatology, and bestowal of the Physician Recognition Award by the Arthritis Foundation, Massachusetts Chapter, in addition to the receipt of his Guggenheim Fellowship.
Dan Furst, M.D.
Daniel E Furst, M.D., is the Carl M Pearson Professor of Medicine at the University of California Los Angeles (UCLA) Medical Center, David Geffen School of Medicine, Division of Rheumatology. He earned his medical degree from Johns Hopkins University, where he also completed his internship and residency. After serving as Assistant Professor of Medicine/Rheumatology at the UCLA Medical Center and as Associate Professor of Internal Medicine/Rheumatology at the University of Iowa Carver College of Medicine, he became Clinical Professor in the Department of Medicine, Division of Rheumatology and Connective Tissue Research at the University of Medicine and Dentistry of New Jersey. He later served as Director of Clinical Research Programs and the Arthritis Clinical Research Unit at the Virginia Mason Medical Center in Seattle, WA. He has served on a number of national committees, and was a fellow in the American College of Rheumatology and The American Society of Clinical Pharmacology and Therapeutics. He has also been a member of the Arthritis Advisory Committee for the U.S. Food and Drug Administration. He has served on the editorial boards of Inpharma, Clinical Drug Investigation, Drugs, The Journal of Clinical Rheumatology, and The Journal of Rheumatology. Additionally, he is an editorial reviewer for professional publications including Arthritis & Rheumatism, The New England Journal of Medicine, Journal of Clinical Investigation, Pharmacotherapy, and the Annals of the Rheumatic Diseases. His research interests include the clinical pharmacology of anti-rheumatic drugs and biologics, and the pathophysiology and treatment of systemic sclerosis.
50
Table of Contents
Michael Knowles, M.D., Ph.D.
Dr. Michael Knowles is a Professor of Pulmonary and Critical Care medicine at the University of North Carolina. He has over three decades of clinical research experience that spans across the disciplines of biology, physiology and the design of clinical trials in both the academic and private sectors. He is currently the head of two large multicenter studies: 1) Genetic Modifiers of Disease phenotype (severity) in cystic fibrosis lung and liver disease, which also includes a recently-formed International Consortium doing a whole genome scan; and 2) a consortium with eight sites in North America to study rare genetic disorders of mucociliary clearance.
Code of Business Conduct and Ethics
We have adopted a written code of business conduct and ethics that applies to our employees, officers and directors. A copy of the code is posted on the Corporate Governance section of our website, which is located at www.corbuspharma.com. We intend to disclose future amendments to certain provisions of our code of business conduct and ethics, or waivers of such provisions applicable to any principal executive officer, principal financial officer, principal accounting officer or controller, or persons performing similar functions, and our directors, on our website identified above or in a current report on Form 8-K.
Limitation of Directors Liability and Indemnification
The Delaware General Corporation Law authorizes corporations to limit or eliminate, subject to certain conditions, the personal liability of directors to corporations and their stockholders for monetary damages for breach of their fiduciary duties. Our certificate of incorporation limits the liability of our directors to the fullest extent permitted by Delaware law. In addition, we have entered into indemnification agreements with certain of our directors and officers whereby we have agreed to indemnify those directors and officers to the fullest extent permitted by law, including indemnification against expenses and liabilities incurred in legal proceedings to which the director or officer was, or is threatened to be made, a party by reason of the fact that such director or officer is or was a director, officer, employee or agent of the Company, provided that such director or officer acted in good faith and in a manner that the director or officer reasonably believed to be in, or not opposed to, the best interests of the Company.
We have director and officer liability insurance to cover liabilities our directors and officers may incur in connection with their services to us, including matters arising under the Securities Act. Our certificate of incorporation and bylaws also provide that we will indemnify our directors and officers who, by reason of the fact that he or she is one of our officers or directors of our company, is involved in any action, suit or proceeding, whether civil, criminal, administrative or investigative related to their board role with the company.
There is no pending litigation or proceeding involving any of our directors, officers, employees or agents in which indemnification will be required or permitted. We are not aware of any threatened litigation or proceeding that may result in a claim for such indemnification.
51
Table of Contents
Summary Compensation Table
The following table presents information regarding the total compensation awarded to, earned by, or paid to our chief executive officer and the two most highly-compensated executive officers (other than the chief executive officer) who were serving as executive officers as of December 31, 2014 for services rendered in all capacities to us for the year ended December 31, 2014. These individuals are our named executive officers for 2014.
| Name and Principal Position |
Year | Salary ($)(2) |
Bonus ($) |
Stock Awards ($) |
Option Awards ($) (1) |
Non-equity Incentive Plan Compensation ($) |
All Other Compensation ($) |
Total ($) | ||||||||||||||||||||||
| Yuval Cohen |
2014 | $ | 174,989 | 45,000 | (3) | $ | 681,672 | $ | | $ | | $ | 901,661 | |||||||||||||||||
| Chief Executive Officer |
||||||||||||||||||||||||||||||
| Mark Tepper |
2014 | 211,060 | | 345,599 | | | 556,659 | |||||||||||||||||||||||
| President and Chief Scientific Officer |
||||||||||||||||||||||||||||||
| Sean Moran |
2014 | 145,643 | 20,000 | (3) | 229,960 | | | 395,603 | ||||||||||||||||||||||
| Chief Financial Officer |
||||||||||||||||||||||||||||||
| (1) | Amounts reflect the grant date fair value of option awards granted in 2014 in accordance with Accounting Standards Codification Topic 718. For information regarding assumptions underlying the valuation of equity awards, see Note 3 to our Consolidated Financial Statements and the discussion under Managements Discussion and Analysis of Financial Condition and Results of OperationsApplication of Critical Accounting Policies and Significant EstimatesStock-Based Compensation included in our Annual Report on Form 10-K for the fiscal year ended December 31, 2014. These amounts do not correspond to the actual value that may be received by the named executive officers if the stock options are exercised. |
| (2) | Each of the named executive officers began receiving salary on April 11, 2014. |
| (3) | Represents signing bonus paid. |
Employment Agreements with Our Named Executive Officers
On April 11, 2014, the closing date of the Merger, we entered into an employment agreement with Dr. Yuval Cohen, which is effective for a period of two years. Dr. Cohens employment agreement provides for him to serve as Chief Executive Officer and provides for an annual base salary of $240,000 and a signing bonus of $45,000. In addition, Dr. Cohen is eligible to receive an annual bonus, which is targeted at up to 33% of his base salary but which may be adjusted by our board of directors based on his individual performance and our performance as a whole. On April 11, 2014, Dr. Cohen received a grant of options covering 312,728 shares of common stock at an exercise price of $1.00 per share. These options vest 25% on the one year anniversary of the grant date and the remainder in equal monthly installments over three years, with full acceleration of vesting on a change in control (as defined in our 2014 Equity Compensation Plan). Dr. Cohen is subject to non-compete and non-solicitation provisions, which apply during the term of his employment and for a period of twelve months following termination of his employment. In addition, the employment agreement contains customary confidentiality and assignment of inventions provisions. If we terminate Dr. Cohens employment without cause or he terminates his employment for good reason, we are required to pay him as severance twelve months of his base salary plus reimbursement of health coverage for twelve months, and he may be paid a pro-rated bonus, each subject to his timely execution of a general release and continuing compliance with covenants. Dr. Cohens severance payments and other applicable payments and benefits will be subject to reduction to the extent doing so would put him in a better after-tax position after taking into account any excise tax he may incur under Internal Revenue Code Section 4999 in connection with any change in control of us or his subsequent termination of employment.
On April 11, 2014, the closing date of the Merger, we entered into an employment agreement with Sean Moran, which we amended and restated on June 26, 2014. Mr. Morans employment agreement provides for him to serve as Chief Financial Officer and provides for an
52
Table of Contents
annual base salary of $200,000 and a signing bonus of $20,000. In addition, Mr. Moran is eligible to receive an annual bonus, which is targeted at up to 33% of his base salary but which may be adjusted by our board of directors based on his individual performance and our performance as a whole. Mr. Morans employment agreement is on an at will basis for an indefinite term. On April 11, 2014, Mr. Moran, received a grant of options covering 107,220 shares of common stock at an exercise price of $1.00 per share. These options vest 25% on the one year anniversary of the grant date and the remainder in equal monthly installments over three years, with full acceleration of vesting on a change in control (as defined in our 2014 Equity Compensation Plan). Mr. Moran is subject to non-compete and non-solicitation provisions, which apply during the term of his employment and for a period of twelve months following termination of his employment. In addition, the employment agreement contains customary confidentiality and assignment of inventions provisions. Mr. Morans applicable payments and benefits will be subject to reduction to the extent doing so would put him in a better after-tax position after taking into account any excise tax he may incur under Internal Revenue Code Section 4999 in connection with any change in control of us or his subsequent termination of employment.
On April 11, 2014, the closing date of the Merger, we entered into an employment agreement with Dr. Mark Tepper, which is effective for a period of two years. Dr. Teppers employment agreement provides for him to serve as President and Chief Scientific Officer and provides for an annual base salary of $240,000. In addition, Dr. Tepper is eligible to receive an annual bonus, which is targeted at up to 33% of his base salary but which may be adjusted by our board of directors based on his individual performance and our performance as a whole. On April 11, 2014, Dr. Tepper received a grant of options covering 271,600 shares of common stock at an exercise price of $1.00 per share. These options vest 25% on the one year anniversary of the grant date and the remainder in equal monthly installments over three years, with full acceleration of vesting on a change in control (as defined in our 2014 Equity Compensation Plan). Dr. Tepper is subject to non-compete and non-solicitation provisions, which apply during the term of his employment and for a period of twelve months following termination of his employment. In addition, the employment agreement contains customary confidentiality and assignment of inventions provisions. If we terminate Dr. Teppers employment without cause or he terminates his employment for good reason, we are required to pay him as severance twelve months of his base salary plus reimbursement of health coverage for twelve months, and he may be paid a pro-rated bonus, each subject to his timely execution of a general release and continuing compliance with covenants. Dr. Teppers severance payments and other applicable payments and benefits will be subject to reduction to the extent doing so would put him in a better after-tax position after taking into account any excise tax he may incur under Internal Revenue Code Section 4999 in connection with any change in control of us or his subsequent termination of employment.
We have entered into a letter agreement with Barbara White, M.D. Dr. Whites letter agreement provides for her to serve as Chief Medical Officer and provides for an annual base salary of $300,000. In addition, Dr. White is eligible to receive an annual bonus, which is targeted at up to 33% of her base salary but which may be adjusted by our board of directors based on her individual performance and our performance as a whole. Dr. Whites letter agreement is on an at will basis for an indefinite term. On September 23, 2014, Dr. White received a grant of options covering 250,000 shares of common stock at an exercise price of $1.00 per share. These options vest 25% on the one year anniversary of the grant date and the remainder in equal monthly installments over three years, with full acceleration of vesting on a change in control (as defined in our 2014 Equity Compensation Plan). Dr. White is subject to non-compete and non-solicitation provisions, which apply during the term of her employment. In addition, the letter agreement contains customary confidentiality and assignment of inventions provisions.
53
Table of Contents
Outstanding Equity Awards at Fiscal Year-End
The following table summarizes, for each of the named executive officers, the number of shares of common stock underlying outstanding stock options held as of December 31, 2014.
|
Number of securities underlying unexercised options (#) |
Equity Incentive Plan Awards: Number of Securities Underlying Unexercised Unearned Options (#) |
Option Exercise Price ($) |
Option Expiration Date |
|||||||||||||||||
| Name |
Exercisable | Unexercisable | ||||||||||||||||||
| Yuval Cohen |
15,089 | (1) | $ | 0.17 | 7/1/2023 | |||||||||||||||
| 215,384 | (2) | $ | 0.17 | 1/28/2024 | ||||||||||||||||
| 312,728 | (3) | $ | 1.00 | 4/11/2024 | ||||||||||||||||
| 700,000 | (4) | 350,000 | (4) | $ | 1.00 | 10/22/2024 | ||||||||||||||
| Mark Tepper |
150,889 | (5) | $ | 0.11 | 7/1/2020 | |||||||||||||||
| 271,600 | (3) | $ | 1.00 | 4/11/2024 | ||||||||||||||||
| 300,000 | (4) | 150,000 | (4) | $ | 1.00 | 10/22/2024 | ||||||||||||||
| Sean Moran |
73,846 | (2) | $ | 0.17 | 1/28/2024 | |||||||||||||||
| 107,220 | (3) | $ | 1.00 | 4/11/2024 | ||||||||||||||||
| 235,000 | (4) | 117,500 | (4) | $ | 1.00 | 10/22/2024 | ||||||||||||||
(1) Represents options to purchase shares of our common stock granted on July 1, 2013. The shares underlying the option vested in 12 equal monthly installments commencing on July 1, 2013.
(2) Represents options to purchase shares of our common stock granted on January 28, 2014. 25% of the option vested on January 28, 2015, with the remaining 75% of the option vesting in equal monthly installments over a period of 36 months commencing on January 28, 2015.
(3) Represents options to purchase shares of our common stock granted on April 11, 2014. 25% of these option vests on April 11, 2015, with the remaining 75% of the option vesting in equal monthly installments over a period of 36 months commencing on April 11, 2015.
(4) Represents options to purchase shares of our common stock granted on October 22, 2014. 12.5% of these option vests on October 22, 2015 and 37.5% of the option vests in equal monthly installments over a period of 36 months commencing on October 22, 2015. The remaining 50% of the option vests in tranches between 5% and 10% upon the achievement of eight individual business milestones.
(5) Represents options to purchase shares of our common stock granted on July 1, 2010. 25% of the option vested on grant date and 12.5% of the remaining portion of the option vested in equal quarterly installments over a period of six quarters.
Director Compensation
The following table sets forth information concerning the compensation paid to our non-employee directors during the fiscal year ended December 31, 2014.
| Name |
Fees Earned or Paid in Cash ($) |
Option Awards ($)(1) |
Total ($) |
|||||||||
| Alan Holmer |
26,250 | 23,591 | 49,841 | |||||||||
| Avery Catlin |
15,417 | 21,768 | 37,185 | |||||||||
| David Hochman |
18,750 | 22,066 | 40,816 | |||||||||
| Renu Gupta |
16,667 | 22,066 | 38,733 | |||||||||
54
Table of Contents
| (1) | Amounts reflect the aggregate grant date fair value of each stock option granted in 2014, in accordance with the Accounting Standards Codification Topic 718. For information regarding assumptions underlying the valuation of equity awards, see Note 3 to our Consolidated Financial Statements and the discussion under Managements Discussion and Analysis of Financial Condition and Results of OperationsApplication of Critical Accounting Policies and Significant EstimatesStock-Based Compensation included in this prospectus. These amounts do not correspond to the actual value that may be received by the directors if the stock options are exercised. |
| (2) | The aggregate number of shares of common stock underlying stock options outstanding as of December 31, 2014 held by Mr. Holmer was 68,861. |
| (3) | The aggregate number of shares of common stock underlying stock options outstanding as of December 31, 2014 held by Mr. Catlin was 50,000. |
| (4) | The aggregate number of shares of common stock underlying stock options outstanding as of December 31, 2014 held by Mr. Hochman was 50,000. |
| (5) | The aggregate number of shares of common stock underlying stock options outstanding as of December 31, 2014 held by Dr. Gupta was 50,000. |
Non-Employee Director Compensation Policy
On July 9, 2014, our board of directors approved a director compensation policy for our non-employee directors. Other than reimbursement for reasonable expenses incurred in connection with attending board of director and committee meetings, this policy excludes any non-employee directors designated to the board by our current investors. This policy provides for the following cash compensation:
| | each non-employee director is entitled to receive an annual fee from us of $25,000; |
| | the chair of our audit committee will receive an annual fee from us of $10,000; |
| | the chair of our compensation committee will receive an annual fee from us of $5,000; and |
| | the chair of our nominating and corporate governance committee will receive an annual fee from us of $5,000. |
Each non-employee director that joins our board of directors receives an initial option grant to purchase 50,000 shares of our common stock under our existing equity incentive plan, or any other equity incentive plan we may adopt in the future, which shall vest in 24 equal monthly installments, the first vesting date to occur on the one-month anniversary of the grant date. Each non-employee director also receives an annual option grant to purchase 20,000 shares of our common stock under our existing equity incentive plan, or any other equity incentive plan we may adopt in the future, which shall vest in 24 equal monthly installments, the first vesting date to occur on the one-month anniversary of the grant date. Upon a change in control, as defined in our equity incentive plan, 100% of the shares underlying these options shall become vested and exercisable immediately prior to such change in control.
All fees under the director compensation policy will be paid on a quarterly basis in arrears and no per meeting fees will be paid. We will also reimburse non-employee directors for reasonable expenses incurred in connection with attending board of director and committee meetings.
Scientific Advisory Board Compensation
We do not currently have a policy regarding compensation for our scientific advisory board members, however each member of the scientific advisory board has received a payment of $15,000 per year and an initial grant of 30,000 options to purchase shares of our common stock at the fair market value on the date of grant.
2014 Equity Compensation Plan
General
On March 26, 2014, our board of directors adopted the 2014 Equity Compensation Plan, or the 2014 Plan, subject to stockholder approval, which was received on April 1, 2014, pursuant to the terms described herein.
55
Table of Contents
The general purpose of the 2014 Plan is to provide a means whereby eligible employees, officers, non-employee directors and other individual service providers develop a sense of proprietorship and personal involvement in our development and financial success, and to encourage them to devote their best efforts to our business, thereby advancing our interests and the interests of our stockholders. By means of the 2014 Plan, we seek to retain the services of such eligible persons and to provide incentives for such persons to exert maximum efforts for our success and the success of our subsidiaries.
Description of the 2014 Equity Compensation Plan
The following description of the principal terms of the 2014 Plan is a summary and is qualified in its entirety by the full text of the 2014 Plan.
Administration. The 2014 Plan is administered by the Compensation Committee of our board of directors. The Compensation Committee may grant options to purchase shares of our common stock, stock appreciation rights, restricted stock, stock units, performance shares, performance units, incentive bonus awards, other cash-based awards and other stock-based awards. The Compensation Committee also has authority to determine the terms and conditions of each award, prescribe, amend and rescind rules and regulations relating to the 2014 Plan, and amend the terms of awards in any manner not inconsistent with the 2014 Plan (provided that no amendment may adversely affect the rights of a participant without consent). The Compensation Committee may delegate authority to officers to grant options and other awards to employees (other than themselves), subject to applicable law and restrictions in the 2014 Plan. No award may be granted under the 2014 Plan on or after the ten year anniversary of the adoption of the 2014 Plan by our board of directors, but awards granted prior to the ten year anniversary may extend beyond that date.
Eligibility. Persons eligible to receive awards under the 2014 Plan include any person who is an employee, officer, director, consultant, advisor or other individual service provider of our Company or any subsidiary, or any person who is determined by the Compensation Committee to be a prospective employee, officer, director, consultant, advisor or other individual service provider of our Company or any subsidiary.
Shares Subject to the 2014 Plan. The aggregate number of shares of common stock available for issuance in connection with options and awards granted under the 2014 Plan is 6,850,334 shares. Incentive Stock Options may, but need not be, granted with respect to all of the shares available for issuance under the 2014 Plan. If any award granted under the 2014 Plan payable in shares of common stock is forfeited, cancelled, or returned for failure to satisfy vesting requirements, otherwise terminates without payment being made, or if shares of common stock are withheld to cover withholding taxes on options or other awards, the number of shares of common stock as to which such option or award was forfeited, or which were withheld, will be available for future grants under the 2014 Plan.
In addition, the 2014 Plan contains an evergreen provision allowing for an annual increase in the number of shares of our common stock available for issuance under the 2014 Plan on January 1 of each year during the period beginning January 1, 2015, and ending on (and including) January 1, 2024. The annual increase in the number of shares shall be equal to the greater of (i) seven percent (7%) of the total number of shares of our common stock outstanding on December 31st of the preceding calendar year, or (ii) the difference between (x) twenty percent (20%) of the total number of shares of our common stock outstanding on December 31st of the preceding calendar year, and (y) the total number of shares of our common stock reserved under the 2014 Plan on December 31st of such preceding calendar year (including shares subject to outstanding awards, issued pursuant to awards or available for future awards); provided, however, that our board of directors may act prior to the first day of any calendar year to provide that there shall be no increase such calendar year, or that the increase shall be a lesser number of shares of common stock than would otherwise occur.
Terms and Conditions of Options. Options granted under the 2014 Plan may be either incentive stock options that are intended to meet the requirements of Section 422 of the Code or nonqualified stock options that do not meet the requirements of Section 422 of the Code. The Compensation Committee will determine the exercise price of options granted under the 2014 Plan. The exercise price of stock options may not be less than the fair market value per share of our common stock on the date of grant (or 110% of fair market value in the case of incentive stock options granted to a ten-percent stockholder).
If on the date of grant the common stock is listed on a stock exchange or national market system, the fair market value will generally be the closing sale price on the date of grant. If the common stock is not traded on a stock exchange or national market system on the date of grant, the fair market value will generally be the average of the closing bid and asked prices for the common stock on the date of grant. If no such prices are available, the fair market value shall be determined in good faith by the Compensation Committee based on the reasonable application of a reasonable valuation method. Notwithstanding the foregoing, if the date for which fair market value is determined is the date on which the final prospectus relating to an initial public offering of the Company is filed, the fair market value for such date will be the Price to the Public (or equivalent) set forth on the cover page for the final prospectus.
No option may be exercisable for more than ten years from the date of grant (five years in the case of an incentive stock option granted to a ten-percent stockholder). Options granted under the 2014 Plan will be exercisable at such time or times as the Compensation
56
Table of Contents
Committee prescribes at the time of grant. No employee may receive incentive stock options that first become exercisable in any calendar year in an amount exceeding $100,000. The Compensation Committee may, in its discretion, permit a holder of a nonqualified stock option to exercise the option before it has otherwise become exercisable, in which case the shares of our common stock issued to the recipient will be restricted stock subject to vesting requirements analogous to those that applied to the option before exercise.
Generally, the exercise price of an option may be paid (a) in cash or by certified bank check, (b) through delivery of shares of our common stock having a fair market value equal to the purchase price, or (c) such other method as approved by the Compensation Committee and set forth in an award agreement. The Compensation Committee is also authorized to establish a cashless exercise program and to permit the exercise price to be satisfied by reducing from the shares otherwise issuable upon exercise a number of shares having a fair market value equal to the exercise price.
No option may be transferred other than by will or by the laws of descent and distribution, and during a recipients lifetime an option may be exercised only by the recipient. However, the Compensation Committee may permit the holder of nonqualified stock options, share-settled stock appreciation rights, restricted stock, performance shares or other share-settled stock based awards to transfer the option, right or other award to immediate family members, to a trust for estate planning purposes, or by gift to charitable institutions. The Compensation Committee will determine the extent to which a holder of a stock option may exercise the option following termination of service with us.
Stock Appreciation Rights. The Compensation Committee may grant stock appreciation rights independent of or in connection with an option. The Compensation Committee will determine the other terms applicable to stock appreciation rights. The base price of a stock appreciation right will be determined by the Compensation Committee, but will not be less than 100% of the fair market value of a share of our common stock on the date of grant. The maximum term of any SAR granted under the 2014 Plan is ten years from the date of grant. Generally, each SAR will entitle a participant upon exercise to an amount equal to:
| | the excess of the fair market value on the exercise date of one share of our common stock over the base price, multiplied by |
| | the number of shares of common stock as to which the stock appreciation right is exercised. |
Payment may be made in shares of our common stock, in cash, or partly in common stock and partly in cash, all as determined by the Compensation Committee.
Restricted Stock and Stock Units. The Compensation Committee may award restricted common stock and/or stock units under the 2014 Plan. Restricted stock awards consist of shares of stock that are transferred to a participant subject to restrictions that may result in forfeiture if specified conditions are not satisfied. Stock units confer the right to receive shares of our common stock, cash, or a combination of shares and cash, at a future date upon or following the attainment of certain conditions specified by the Compensation Committee. The Compensation Committee will determine the restrictions and conditions applicable to each award of restricted stock or stock units, which may include performance-based conditions. Dividends with respect to restricted stock may be paid to the holder of the shares as and when dividends are paid to stockholders or at the time that the restricted stock vests, as determined by the Compensation Committee. Dividend equivalent amounts may be paid with respect to stock units, and will be subject to the same restrictions on transferability as the stock units with respect to which they were paid. Unless the Compensation Committee determines otherwise, holders of restricted stock will have the right to vote the shares.
Performance Shares and Performance Units. The Compensation Committee may award performance shares and/or performance units under the 2014 Plan. Performance shares and performance units are awards, denominated in either shares or U.S. dollars, which are earned during a specified performance period subject to the attainment of performance criteria, as established by the Compensation Committee. The Compensation Committee will determine the restrictions and conditions applicable to each award of performance shares and performance units.
Incentive Bonus Awards. The Compensation Committee may award incentive bonus awards payable in cash or common stock, as set forth in an award agreement. The Compensation Committee will determine the terms and conditions applicable to each incentive bonus award.
Other Stock-Based and Cash-Based Awards. The Compensation Committee may award other types of equity-based or cash-based awards under the 2014 Plan, including the grant or offer for sale of shares of our common stock that do not have vesting requirements and the right to receive one or more cash payments subject to satisfaction of such conditions as the Compensation Committee may impose.
Section 162(m) Compliance. If stock or cash-based awards are intended to satisfy the conditions for deductibility under Section 162(m) of the Code as performance-based compensation, the performance criteria will be selected from among the following, which may be applied to our Company as a whole, or to any subsidiary or any division or operating unit thereof: (a) pre-tax income; (b) after-tax income; (c) net income; (d) operating income or profit; (e) cash flow, free cash flow, cash flow return on investment (discounted or otherwise), net cash provided by operations, or cash flow in excess of cost of capital; (f) earnings per share (basic or diluted); (g) return on equity; (h) returns on sales or revenues; (i) return on invested capital or assets (gross or net); (j) cash, funds or earnings available for distribution; (k) appreciation in the fair
57
Table of Contents
market value of our common stock; (l) operating expenses; (m) implementation or completion of critical projects or processes; (n) return on investment; (o) total return to stockholders (meaning the aggregate common stock price appreciation and dividends paid (assuming full reinvestment of dividends) during the applicable period); (p) net earnings growth; (q) return measures (including but not limited to return on assets, capital, equity, or sales); (r) increase in revenues; (s) the Companys published ranking against its peer group of pharmaceutical companies based on total stockholder return; (t) net earnings; (u) changes (or the absence of changes) in the per share price of the Companys common stock; (v) clinical or regulatory milestones; (w) earnings before or after any one or more of the following items: interest, taxes, depreciation or amortization, as reflected in the Companys financial reports for the applicable period; (x) total revenue growth (meaning the increase in total revenues after the date of grant of an award and during the applicable period, as reflected in the Companys financial reports for the applicable period); (y) economic value created; (z) operating margin or profit margin; (aa) share price or total shareholder return; (bb) cost targets, reductions and savings, productivity and efficiencies; (cc) strategic business criteria, consisting of one or more objectives based on meeting objectively determinable criteria: specified market penetration, geographic business expansion, investor satisfaction, employee satisfaction, human resources management, supervision of litigation, information technology, and goals relating to acquisitions, divestitures, joint ventures and similar transactions, and budget comparisons; (dd) objectively determinable personal or professional objectives, including any of the following performance goals: the implementation of policies and plans, the negotiation of transactions, the development of long term business goals, formation of joint ventures, research or development collaborations, and the completion of other corporate transactions; and (ee) any combination of, or a specified increase or improvement in, any of the foregoing.
At the end of the performance period established in connection with any award, the Compensation Committee will determine the extent to which the performance goal or goals established for such award have been attained, and shall determine, on that basis, the shares or, if applicable, the cash or other property that has been earned and as to which payment will be made. The Compensation Committee will certify in writing the extent to which it has determined that the performance goal or goals established by it for such award have been attained.
With respect to awards intended to be exempt from the deductibility limitation in Section 162(m) of the Code, no participant in any one fiscal year may be granted (x) stock options or stock appreciation rights with respect to more than 3,000,000 shares of common stock in the aggregate, and (y) restricted stock, stock units, performance shares awards, incentive bonus awards and other stock based awards that are denominated in shares of common stock with respect to more than 3,000,000 shares in the aggregate, and the maximum dollar value payable to any participant in any one (1) fiscal year with respect to stock units, performance units or incentive bonus awards or other stock-based awards that may be settled in cash or other property (other than common stock) is $3,000,000.
Effect of Certain Corporate Transactions. The Compensation Committee may, at the time of the grant of an award, provide for the effect of a change in control (as defined in the 2014 Plan) on any award, including (i) accelerating or extending the time periods for exercising, vesting in, or realizing gain from any award, (ii) eliminating or modifying the performance or other conditions of an award, (iii) providing for the cash settlement of an award for an equivalent cash value, as determined by the Compensation Committee, or (iv) such other modification or adjustment to an award as the Compensation Committee deems appropriate to maintain and protect the rights and interests of participants following a change in control. The Compensation Committee may, in its discretion and without the need for the consent of any recipient of an award, also take one or more of the following actions contingent upon the occurrence of a change in control: (a) cause any or all outstanding options and stock appreciation rights to become immediately exercisable, in whole or in part; (b) cause any other awards to become non-forfeitable, in whole or in part; (c) cancel any option or stock appreciation right in exchange for a substitute option; (d) cancel any award of restricted stock, stock units, performance shares or performance units in exchange for a similar award of the capital stock of any successor corporation; (e) redeem any restricted stock, stock unit, performance share or performance unit for cash and/or other substitute consideration with a value equal to the fair market value of an unrestricted share of our common stock on the date of the change in control; (f) cancel any option or stock appreciation right in exchange for cash and/or other substitute consideration based on the value of our common stock on the date of the change in control , and cancel any option or stock appreciation right without any payment if its exercise price exceeds the value of our common stock on the date of the change in control; or (g) make such other modifications, adjustments or amendments to outstanding awards as the Compensation Committee deems necessary or appropriate.
Amendment, Termination. The Compensation Committee may amend the terms of awards in any manner not inconsistent with the 2014 Plan, provided that no amendment shall adversely affect the rights of a participant with respect to an outstanding award without the participants consent. In addition, our board of directors may at any time amend, suspend, or terminate the 2014 Plan, provided that (i) no such amendment, suspension or termination shall materially and adversely affect the rights of any participant under any outstanding award without the consent of such participant and (ii) to the extent necessary to comply with any applicable law, regulation, or stock exchange rule, the 2014 Plan requires us to obtain stockholder consent. Stockholder approval is required for any plan amendment that increases the number of shares of common stock available for issuance under the 2014 Plan or changes the persons or classes of persons eligible to receive awards.
Tax Withholding
As and when appropriate, we shall have the right to require each optionee purchasing shares of common stock and each grantee receiving an award of shares of common stock under the 2014 Plan to pay any federal, state or local taxes required by law to be withheld.
58
Table of Contents
Option Grants and Stock Awards
The grant of options and other awards under the 2014 Plan will be discretionary and we cannot determine now the specific number or type of options or awards to be granted in the future to any particular person or group. Upon consummation of the Merger, options to purchase up to 905,334 shares of common stock under the 2014 Plan were substituted for outstanding options under the JB Therapeutics, Inc. 2010 Equity Incentive Plan. These options have exercise prices ranging from $0.11 to $0.17. On April 11, 2014, the closing date of the Merger, we issued stock options to purchase up to 691,548 shares at an exercise price of $1.00 per share. On July 11, 2014 and September 23, 2014, we issued stock options to purchase 330,000 and 392,500, respectively, shares at an exercise price of $1.00 per share. On October 22, 2014, we issued stock options to purchase 1,235,000 shares at an exercise price of $1.00.
Option Substitution
Pursuant to the terms of the Merger Agreement, each outstanding option to purchase shares of common stock of JB Therapeutics, Inc. under the JB Therapeutics, Inc. 2010 Equity Incentive Plan was substituted for an option to purchase shares of our Companys common stock under the 2014 Plan, with the number and exercise price of the substituted options determined by applying an exchange ratio. Except for these changes, each substituted option remains subject to substantially the same terms and conditions (including vesting terms) as in effect immediately prior to the Merger. The JB Therapeutics, Inc. 2010 Equity Incentive Plan was terminated upon the Merger, but if any provision of the terminated plan is necessary to give effect to or supply terms of the outstanding option awards, reference may be made to the plan in these limited circumstances.
59
Table of Contents
The following table sets forth information regarding the beneficial ownership of our common stock as of the date of this prospectus by:
| | each person known by us to be the beneficial owner of more than 5% of our outstanding shares of common stock; |
| | each of our named executive officers and directors; and |
| | all of our executive officers and directors as a group. |
Beneficial ownership is determined based on the rules and regulations of the SEC. A person has beneficial ownership of shares if such individual has the power to vote and/or dispose of shares. This power may be sole or shared and direct or indirect. In computing the number of shares beneficially owned by a person and the percentage ownership of that person, shares of common stock that are subject to options or warrants held by that person and exercisable as of, or within 60 days of, March 12, 2015 are counted as outstanding. These shares, however, are not counted as outstanding for the purposes of computing the percentage ownership of any other person(s). Except as may be indicated in the footnotes to this table and pursuant to applicable community property laws, each person named in the table has sole voting and dispositive power with respect to the shares of common stock set forth opposite that persons name. Unless indicated below, the address of each individual listed below is c/o Corbus Pharmaceuticals Holdings, Inc., 100 River Ridge Drive, Norwood, MA 02062.
Applicable percentage ownership in the following table is based on 26,003,304 shares of common stock outstanding as of March 12, 2015. Beneficial ownership representing less than 1% is denoted with an asterisk (*).
| Name of Beneficial Owner |
Number of Shares Beneficially Owned |
Percentage of Shares Beneficially Owned |
||||||
| Officers and Directors |
||||||||
| Mark Tepper (1) |
2,324,847 | 8.9 | % | |||||
| Yuval Cohen (2) |
168,993 | * | ||||||
| Sean Moran (3) |
83,466 | * | ||||||
| Alan Holmer (4) |
59,694 | * | ||||||
| David Hochman (5) |
677,033 | 2.6 | % | |||||
| Renu Gupta (6) |
25,833 | * | ||||||
| Avery W. Catlin (7) |
16,667 | * | ||||||
| All current directors and executive officers as a group |
3,416,145 | 12.8 | % | |||||
| 5% Stockholders |
||||||||
| Sumner Burstein |
3,824,846 | 14.7 | % | |||||
| Knoll Capital Management (8) |
2,750,000 | 10.2 | % | |||||
| Lawrence Allen (9) |
2,923,100 | 10.7 | % | |||||
| Perceptive Advisors (10) |
2,000,000 | 7.4 | % | |||||
| Adam Stern (11) |
1,398,900 | 5.3 | % | |||||
(1) Includes 224,447 shares of common stock issuable upon exercise of outstanding stock options exercisable within 60 days of March 12, 2015. Does not include 498,042 shares of common stock issuable upon exercise of outstanding options that are not exercisable within 60 days of March 12, 2015.
(2) Includes 167,093 shares of common stock issuable upon exercise of outstanding stock options exercisable within 60 days of March 12, 2015. Does not include 1,076,108 shares of common stock issuable upon exercise of outstanding options that are not exercisable within 60 days of March 12, 2015.
(3) Includes 52,116 shares of common stock issuable upon exercise of outstanding stock options exercisable within 60 days of March 12, 2015. Does not include 363,950 shares of common stock issuable upon exercise of outstanding stock options that are not exercisable within 60 days of March 12, 2015.
60
Table of Contents
(4) Includes 39,694 shares of common stock issuable upon exercise of outstanding stock options, and 10,000 shares of common stock issuable upon exercise of outstanding warrants, both of which are exercisable within 60 days of March 12, 2015. Does not include 29,167 shares of common stock issuable upon exercise of outstanding options that are not exercisable within 60 days of March 12, 2015.
(5) Includes 20,833 shares of common stock issuable upon exercise of outstanding stock options, and 10,000 shares of common stock issuable upon exercise of outstanding warrants, both of which are exercisable within 60 days of March 12, 2015. Includes 140,000 shares of common stock, and 50,000 shares of common stock issuable upon exercise of outstanding warrants that are exercisable within 60 days of March 12, 2015 held by a family trust of which Mr. Hochman is a co-trustee and co-beneficiary. Includes 12,900 shares of common stock held by trusts for the benefit of his children of which Mr. Hochman disclaims beneficial ownership. Does not include 29,167 shares of common stock issuable upon exercise of outstanding options that are not exercisable within 60 days of March 12, 2015.
(6) Includes 20,833 shares of common stock issuable upon exercise of outstanding stock options exercisable within 60 days of March 12, 2015. Does not include 29,167 shares of common stock issuable upon exercise of outstanding options that are not exercisable within 60 days of March 12, 2015.
(7) Includes 16,667 shares of common stock issuable upon the exercise of outstanding stock options exercisable within 60 days of March 12, 2015. Does not include 33,333 shares of common stock issuable upon exercise of outstanding options that are not exercisable within 60 days of March 12, 2015.
(8) Includes 1,000,000 shares of common stock, and 1,000,000 shares of common stock issuable upon exercise of outstanding warrants that are exercisable within 60 days of March 12, 2015, which are owned by Europa International, Inc., which is beneficially owned by Knoll Capital Management.
(9) Includes (i) 225,000 shares of common stock, and 100,000 shares of common stock issuable upon exercise of outstanding warrants that are exercisable within 60 days of March 12, 2015, both of which are registered in the name of Mr. Allens individual retirement account, (ii) 100,000 shares of common stock and 100,000 shares of common stock issuable upon exercise of outstanding warrants that are exercisable within 60 days of March 12, 2015, both of which are owned by ACP Partners, LP, which is beneficially owned by Mr. Allen, (iii) 1,100,000 shares of common stock, and 1,100,000 shares of common stock issuable upon outstanding warrants that are exercisable within 60 days of March 12, 2015, which are owned by ACP X, LP, which is beneficially owned by Mr. Allen, and (iv) 98,100 shares of common stock and 100,000 shares of common stock issuable upon outstanding warrants that are exercisable within 60 days of March 12, 2015, which are owned by LGA Investments Family Limited Partnership, which is beneficially owned by Mr. Allen.
(10) Includes (i) 870,000 shares of common stock and 870,000 shares of common stock issuable upon exercise of outstanding warrants that are exercisable within 60 days of March 12, 2015, which are owned by Perceptive Life Sciences Master Fund, Ltd., which is beneficially owned by Perceptive Advisors, and (ii) 130,000 shares of common stock and 130,000 shares of common stock issuable upon exercise of outstanding warrants that are exercisable within 60 days of March 12, 2015, which are owned by Titan Perc, Ltd., which is beneficially owned by Perceptive Advisors.
(11) Includes 200,000 shares of common stock issuable upon exercise of outstanding warrants that are exercisable within 60 days of March 12, 2015. Mr. Stern is an affiliate of the Placement Agent. Does not include up to 2,047,000 shares of common stock issuable upon exercise of Warrants issued to the Placement Agent. Mr. Stern disclaims ownership of such shares except to the extent of his pecuniary interest therein.
61
Table of Contents
CERTAIN RELATIONSHIPS AND RELATED PARTY TRANSACTIONS
Other than compensation arrangements for our named executive officers and directors, we describe below each transaction or series of similar transactions, since January 1, 2011, to which we were a party or will be a party, in which:
| | the amounts involved exceeded or will exceed $120,000; and |
| | any of our directors, executive officers or holders of more than 5% of our capital stock, or any member of the immediate family of the foregoing persons, had or will have a direct or indirect material interest. |
Compensation arrangements for our named executive officers and directors are described in the section entitled executive compensation.
The Placement Agent and Related Parties
In connection with the formation of Holdings in December 2013, certain affiliates of the Placement Agent and certain other parties not affiliated with us or the Placement Agent subscribed for an aggregate of 6,000,000 shares of common stock for which they paid an aggregate of $120,000 ($0.02 per share), including David Hochman, one of our directors who purchased 450,000 shares and whose family trust purchased 90,000 shares.
Following the Initial Closing of the 2014 Private Placement, the Placement Agent has a right to appoint one member of our board of directors for a two-year term (the Aegis Nominee). Upon the Initial Closing on April 11, 2014, David Hochman was appointed as the Aegis Nominee and his successor, if any, will be chosen by the Placement Agent, subject to the reasonable approval of the Company and the terms of the Voting Agreement described below.
Consulting Agreement with Orchestra Medical Ventures
On March 21, 2014, Holdings entered into a consulting agreement with Orchestra Medical Ventures, LLC, or Orchestra, of which David Hochman is Managing Partner. The agreement became effective upon closing of the Merger and provides that Orchestra will render a variety of consulting and advisory services relating principally to identifying and evaluating strategic relationships, licensing opportunities, and business strategies. Orchestra is compensated at the rate of $5,000 per month for twelve months, payable quarterly in advance. The consulting agreement will expire on April 11, 2015.
Voting Agreement
In connection with the Initial Closing, the stockholders of JB Therapeutics prior to the Merger, or the JBT Stockholders, and the stockholders of Holdings prior to the Merger and this Offering, or the Holdings Stockholders, entered into a Voting Agreement, or the Voting Agreement. Pursuant to the terms of the Voting Agreement, (i) the JBT Stockholders have the right to nominate three (3) members to our Board, (ii) the Holdings Stockholders shall vote in favor of the election of the JBT Stockholders Nominees and (iii) the Holdings Stockholders shall nominate and vote for one Aegis Nominee to our Board, and (iv) the JBT Stockholders shall vote in favor of the election of the Aegis Nominee. The Voting Agreement expires upon the earlier of (i) the approval of at least 75% of the JBT Stockholders and the Holdings Stockholders voting together based upon their ownership of our common stock, or (ii) the closing of a firm commitment underwritten public offering of shares of our common stock resulting in gross proceeds of at least $20 million.
Indemnification Agreements
In September 2014, we entered into indemnification agreements with certain of our directors and officers. For more information, see the description of the indemnification agreements under Executive Compensation -Limitation of Directors Liability and Indemnification.
Merger Transaction
On March 27, 2014, JB Therapeutics entered into the Merger Agreement with Merger Sub, a wholly-owned subsidiary of Holdings. Pursuant to the terms of the Merger Agreement, as a condition of and contemporaneously with the closing of the Merger on April 11, 2014, Merger Sub merged with and into JB Therapeutics and JB Therapeutics became a wholly-owned subsidiary of Holdings. In connection with the Merger, JB Therapeutics changed its name to Corbus Pharmaceuticals, Inc.
62
Table of Contents
While we believe that all of these agreements and arrangements are in the best interests of our Company, related parties of the Placement Agent may derive material benefits as the result of these transactions. In addition, related parties of the Placement Agent will have a continuing substantial interest in our Company and will derive substantial benefits from any success of our Company.
Policies and Procedures for Related Party Transactions
Our board of directors has adopted a policy that our executive officers, directors, nominees for election as a director, beneficial owners of more than 5% of any class of our common stock, any members of the immediate family of any of the foregoing persons and any firms, corporations or other entities in which any of the foregoing persons is employed or is a partner or principal or in a similar position or in which such person has a 5% or greater beneficial ownership interest, which we refer to collectively as related parties, are not permitted to enter into a transaction with us without the prior consent of our board of directors acting through the audit committee or, in certain circumstances, the chairman of the audit committee. Any request for us to enter into a transaction with a related party, in which the amount involved exceeds $100,000 and such related party would have a direct or indirect interest must first be presented to our audit committee, or in certain circumstances the chairman of our audit committee, for review, consideration and approval. In approving or rejecting any such proposal, our audit committee, or the chairman of our audit committee, is to consider the material facts of the transaction, including, but not limited to, whether the transaction is on terms no less favorable than terms generally available to an unaffiliated third party under the same or similar circumstances, the extent of the benefits to us, the availability of other sources of comparable products or services and the extent of the related partys interest in the transaction.
63
Table of Contents
Our current certificate of incorporation, as amended, authorizes us to issue:
| | 150,000,000 shares of common stock, par value $0.0001 per share; and |
| | 10,000,000 shares of Preferred Stock, par value $0.0001 per share, none of which have yet been designated. |
As of March 12, 2015, there were 26,003,304 shares of common stock outstanding and no shares of preferred stock outstanding.
Reverse Stock Split Range Authorization
Our board of directors and stockholders have approved a reverse stock split within a range of 1:1.25 to 1:5 (the reverse stock split range).
The following statements are summaries only of provisions of our authorized capital stock and are qualified in their entirety by our certificate of incorporation, as amended. You should review these documents for a description of the rights, restrictions and obligations relating to our capital stock. Copies of our certificate of incorporation may be obtained from the Company upon written request. For a description of our common stock, see Description of Securities Common Stock below.
Common stock
Voting. The holders of our common stock are entitled to one vote for each share held of record on all matters on which the holders are entitled to vote (or consent pursuant to written consent).
Dividends. The holders of our common stock are entitled to receive, ratably, dividends only if, when and as declared by our board of directors out of funds legally available therefor and after provision is made for each class of capital stock having preference over the common stock.
Liquidation Rights. In the event of our liquidation, dissolution or winding-up, the holders of our common stock are entitled to share, ratably, in all assets remaining available for distribution after payment of all liabilities and after provision is made for each class of capital stock having preference over the common stock.
Conversion Right. The holders of our common stock have no conversion rights.
Preemptive and Similar Rights. The holders of our common stock have no preemptive or similar rights.
Redemption/Put Rights. There are no redemption or sinking fund provisions applicable to the common stock. All of the outstanding shares of our common stock are fully-paid and nonassessable.
Preferred Stock
We are authorized to issue up to 10,000,000 shares of preferred stock, par value $0.0001 per share, with such designations, rights, and preferences as may be determined from time to time by our board of directors. Accordingly, our board of directors is empowered, without stockholder approval, to issue preferred stock with dividend, liquidation, conversion, voting, or other rights that could adversely affect the voting power or other rights of the holders of our common stock. The issuance of preferred stock could have the effect of restricting dividends on our common stock, diluting the voting power of our common stock, impairing the liquidation rights of our common stock, or delaying or preventing a change in control of our company, all without further action by our stockholders. We have no shares of our preferred stock outstanding.
Warrants
Investor Warrants. In connection with our 2014 Private Placement, we issued warrants to investors to purchase an aggregate 10,260,000 shares of our common stock. We refer to these warrants as the Investor Warrants. The Investor Warrants are exercisable for our common stock at an exercise price equal to $1.00 per share (the Exercise Price). The Investor Warrants are exercisable immediately upon issuance and may be exercised for a period of five years from grant. The Investor Warrants may be exercised at any time in whole or in part at the applicable exercise price until expiration of the Investor Warrants. No fractional shares will be issued upon the exercise of the Investor Warrants.
64
Table of Contents
Merger Warrants. In connection with the Merger, we issued warrants to purchase 917,612 shares of our common stock at an exercise price of $1.00 per share to holders of JB Therapeutics Series A Preferred Stock. The Merger Warrants substantially similar terms as the Investor Warrants.
Replacement Warrants. In connection with the Merger, we issued warrants to purchase 27,839 shares of our common stock at an exercise price of $0.60 per share to the existing holders of warrants in JB Therapeutics. The Replacement Warrants are subject to substantially similar terms as the Investor Warrants. We also issued warrants, or the Additional Replacement Warrants, to purchase 350,000 shares of our common stock, with an exercise price of $0.66, to replace previously held warrants to purchase common stock of JB Therapeutics. The Additional Replacement Warrants are substantially similar to the Investor Warrants except that they include cashless exercise provisions and are not subject to redemption by us.
Placement Agent Warrants. In connection with completion of the 2014 Private Placement, we issued Aegis Capital warrants for 2,047,000 shares of our common stock at an exercise price of $1.00 to the Placement Agent as partial compensation. These warrants have a five year term and provide cashless exercise.
Registration Rights
In connection with the 2014 Private Placement, we entered into a registration rights agreement with the private placement investors, the placement agent and the holders of our outstanding warrants. We were required to file with the SEC no later than July 29, 2014 (the Filing Deadline), a registration statement covering the resale of the shares of common stock and the shares of common stock underlying the warrants, issued in the 2014 Private Placement, as well as the shares of common stock underlying the formation warrants, the merger warrants, the replacement warrants, the additional replacement warrants and the private placement warrants. We are also required to use commercially reasonable efforts to have the registration statement declared effective within one hundred and fifty (150) days after the registration statement is filed, or the Effectiveness Deadline, and to keep the registration statement continuously effective under the Securities Act of 1933, as amended, or the Securities Act, until the earlier of the date when all the registrable securities covered by the registration statement have been sold or such time as all of the registrable securities covered by the registration statement can be sold under Rule 144 without any volume limitations.
If this registration statement is not declared effective on or before the Effectiveness Deadline, we will be required to pay to each holder of registrable securities purchased in the 2014 Private Placement an amount in cash equal to one-half of one percent (0.5%) of such holders investment amount on every thirty (30) day anniversary of such Effectiveness Deadline until such failure is cured. The payment amount shall be prorated for partial thirty (30) day periods. The maximum aggregate amount of payments to be made by us as the result of such failure, shall be an amount equal to 6% of each holders investment amount. Notwithstanding the foregoing, no payments shall be owed with respect to any period during which all of the holders registrable securities may be sold by such holder without restriction under Rule 144.
We shall keep the registration statement evergreen for one (1) year from the date it is declared effective by the SEC or until Rule 144 of the Securities Act is available to the holders of registrable securities purchased in the 2014 Private Placement with respect to all of their shares, whichever is earlier.
We will pay all costs and expenses incurred by us in complying with our obligations to file registration statements pursuant to the registration rights agreement, except that the selling holders will be responsible for their shares of the attorneys fees and expenses and any commissions or other compensation to selling agents and similar persons; provided, however, that, in any registration, each party will pay for its own underwriting discounts and commissions and transfer taxes.
Lock-Up Agreements
Each of our directors and officers and the holders of substantially all of 5% or more of our common stock have agreed that they will not (a) offer, sell, contract to sell, grant any option to purchase, hypothecate, pledge or otherwise dispose of or (b) transfer title to any shares of common stock acquired prior to the 2014 Private Placement, which includes any shares of common stock acquired upon the exercise of any warrants acquired prior to the 2014 Private Placement, for a period beginning on April 11, 2014 and ending on the earlier of (i) nine months following the effective date of the registration statement of which this prospectus is a part or (ii) twelve months from May 30, 2014, without the prior written consent of both the Company and Aegis Capital.
From and after the effective date of the registration statement of which this prospectus forms a part, or the Effective Date, the investors in the 2014 Private Placement have agreed that they will not sell, offer, pledge, contract to sell, grant any option or contract to
65
Table of Contents
purchase, lend or otherwise transfer or encumber, directly or indirectly, any shares acquired in the private placement nor will they enter into any swap, hedging or other arrangement that transfers to another, in whole or in part, any of the economic consequences of ownership of any shares acquired in the private placement until the Release Date (defined below), provided that each investor may transfer up to one third of such shares held as of the date of this prospectus at any time on or after such date. The Release Date means April 4, 2015. Following the Release Date, the investors may sell the remaining registrable shares that they hold.
Transfer Agent and Registrar
Continental Stock Transfer & Trust Company, located at 17 Battery Place, 8th Floor, New York, NY 10004, is the transfer agent and registrar for our common stock.
Quotation of Securities
Our common stock is quoted on the Over-the-Counter Markets, or OTC.QB, under the symbol CRBP. Our shares of common stock began being quoted on the OTC.QB under the symbol CRBP effective October 24, 2014.
Anti-Takeover Effect of Delaware Law, Certain Charter and Bylaw Provisions
Our certificate of incorporation and bylaws contain provisions that could have the effect of discouraging potential acquisition proposals or tender offers or delaying or preventing a change of control of our company. These provisions are as follows:
| | they provide that special meetings of stockholders may be called by the board of directors or at the request in writing by stockholders of record owning at least twenty (20%) percent of the issued and outstanding voting shares of common stock; |
| | they do not include a provision for cumulative voting in the election of directors. Under cumulative voting, a minority stockholder holding a sufficient number of shares may be able to ensure the election of one or more directors. The absence of cumulative voting may have the effect of limiting the ability of minority stockholders to effect changes in our board of directors; and |
| | they allow us to issue, without stockholder approval, up to 10,000,000 shares of preferred stock that could adversely affect the rights and powers of the holders of our common stock. |
We are subject to the provisions of Section 203 of the General Corporation Law of the State of Delaware, an anti-takeover law. In general, Section 203 prohibits a publicly held Delaware corporation from engaging in a business combination with an interested stockholder for a period of three years after the date of the transaction in which the person became an interested stockholder, unless the business combination is approved in the following prescribed manner:
| | prior to the time of the transaction, the board of directors of the corporation approved either the business combination or the transaction which resulted in the stockholder becoming an interested stockholder; |
| | upon completion of the transaction that resulted in the stockholder becoming an interested stockholder, the stockholder owned at least 85% of the voting stock of the corporation outstanding at the time the transaction commenced, excluding for purposes of determining the number of shares outstanding (1) shares owned by persons who are directors and also officers and (2) shares owned by employee stock plans in which employee participants do not have the right to determine confidentially whether shares held subject to the plan will be tendered in a tender or exchange offer; and |
| | on or subsequent to the time of the transaction, the business combination is approved by the board and authorized at an annual or special meeting of stockholders, and not by written consent, by the affirmative vote of at least 66 2/3% of the outstanding voting stock which is not owned by the interested stockholder. |
Generally, for purposes of Section 203, a business combination includes a merger, asset or stock sale, or other transaction resulting in a financial benefit to the interested stockholder. An interested stockholder is a person who, together with affiliates and associates, owns or, within three years prior to the determination of interested stockholder status, owned 15% or more of a corporations outstanding voting securities.
66
Table of Contents
Stockholder Action by Written Consent
Our certificate of incorporation, as amended, provides that any action required by law to be taken at any annual or special meeting of the stockholders or any action which may be taken at such a meeting may be taken without a meeting by written consent of the stockholders in lieu of a meeting.
Choice of Forum
Our certificate of incorporation, as amended, provides that, unless we consent in writing to the selection of an alternative forum, the Court of Chancery of the State of Delaware will be the exclusive forum for any derivative action or proceeding brought on our behalf; any action asserting a breach of fiduciary duty; any action asserting a claim against us arising pursuant to the Delaware General Corporation Law, our certificate of incorporation, as amended, or our bylaws; or any action asserting a claim against us that is governed by the internal affairs doctrine.
67
Table of Contents
The following table sets forth information as of the date of this prospectus, to our knowledge, about the beneficial ownership of our common stock by the selling stockholders both before and immediately after the 2014 Private Placement.
All of the selling stockholders received their securities in: (i) our formation and (ii) the 2014 Private Placement; in each case prior to the initial filing date of the registration statement of which this prospectus is a part. We believe that the selling stockholders have sole voting and investment power with respect to all of the shares of common stock beneficially owned by them unless otherwise indicated.
Certain of the selling stockholders and intermediaries, who are identified as broker-dealers in the footnotes to the selling stockholder table, through whom such securities are sold are deemed underwriters within the meaning of the Securities Act of 1933, as amended, with respect to the securities offered hereby, and any profits realized or commissions received may be deemed underwriting compensation. We believe that all securities purchased by broker-dealers or affiliates of broker-dealers were purchased by such persons and entities in the ordinary course of business and at the time of purchase, such purchasers did not have any agreements or understandings, directly or indirectly, with any person to distribute such securities.
The percent of beneficial ownership for the selling stockholders is based on 26,003,304 shares of common stock outstanding as of March 12, 2015. Warrants to purchase shares of our common stock held by certain investors that are currently exercisable or exercisable within 60 days of the date of this prospectus are considered outstanding and beneficially owned by such investors for the purpose of computing the percentage ownership of their respective percentage ownership but are not treated as outstanding for the purpose of computing the percentage ownership of any other stockholder. Unless otherwise stated below, to our knowledge, none of the selling stockholders has had a material relationship with us other than as a stockholder at any time within the past three years or has ever been one of our officers or directors.
Pursuant to Rules 13d-3 and 13d-5 of the Exchange Act, beneficial ownership includes any shares of our common stock as to which a stockholder has sole or shared voting power or investment power, and also any shares of our common stock which the stockholder has the right to acquire within 60 days, including upon exercise of warrants to purchase shares of our common stock.
The shares of common stock being offered pursuant to this prospectus may be offered for sale from time to time during the period the registration statement of which this prospectus is a part remains effective, by or for the account of the selling stockholders. After the date of effectiveness, the selling stockholders may have sold or transferred, in transactions covered by this prospectus or in transactions exempt from the registration requirements of the Securities Act, some or all of their common stock.
Information about the selling stockholders may change over time. Any changed information will be set forth in an amendment to the registration statement or supplement to this prospectus, to the extent required by law.
|
Shares Beneficially Owned as of the date of this Prospectus |
Shares Offered by this Prospectus |
Shares Beneficially Owned After the Offering (1)(2) |
||||||||||||||||||
| Name of Selling Stockholder |
Number | Percent | Number | Percent | ||||||||||||||||
| Europa International, Inc. (3) |
2,750,000 | 10.18 | % | 2,000,000 | 750,000 | 2.88 | % | |||||||||||||
| ACP X, L.P. (4) |
2,200,000 | 8.11 | % | 2,200,000 | | | ||||||||||||||
| Perceptive Life Sciences Master Fund, Ltd. (5) |
1,740,000 | 6.48 | % | 1,740,000 | | | ||||||||||||||
| Lester Petracca |
1,000,000 | 3.77 | % | 1,000,000 | | | ||||||||||||||
| Bobcat Property Trust of Angel Fire, New Mexico (6) |
700,000 | 2.66 | % | 700,000 | | | ||||||||||||||
| Keith Murphy |
625,000 | 2.38 | % | 500,000 | 125,000 | * | ||||||||||||||
| Dina Morrissey |
500,100 | 1.90 | % | 500,000 | 100 | * | ||||||||||||||
| Rexford Capital, LLC (7) |
500,000 | 1.89 | % | 500,000 | | | ||||||||||||||
| Edward M. Dunn |
500,000 | 1.89 | % | 500,000 | | | ||||||||||||||
68
Table of Contents
|
Shares Beneficially Owned as of the date of this Prospectus |
Shares Offered by this Prospectus |
Shares Beneficially Owned After the Offering (1) |
||||||||||||||||||
| Name of Selling Stockholder |
Number | Percent | Number | Percent | ||||||||||||||||
| David Schellhardt |
500,000 | 1.89 | % | 500,000 | | | ||||||||||||||
| Ethan S. Burstein |
498,401 | 1.53 | % | 465,267 | 33,134 | * | ||||||||||||||
| Derek J. Sroufe (8) |
400,000 | 1.53 | % | 100,000 | 300,000 | 1.15 | % | |||||||||||||
| Anup Patel |
348,511 | 1.33 | % | 182,837 | 165,674 | * | ||||||||||||||
| RBC Capital Markets LLC Cust. FBO Laurence G. Allen, IRA (9) |
325,000 | 1.24 | % | 200,000 | 125,000 | * | ||||||||||||||
| SJO Worldwide LLC (10) |
300,000 | 1.11 | % | 300,000 | | | ||||||||||||||
| GJG Life Sciences LLC (11) |
300,000 | 1.11 | % | 300,000 | | | ||||||||||||||
| Titan Perc, Ltd. (12) |
260,000 | * | 260,000 | | | |||||||||||||||
| George Karfunkel |
250,000 | * | 250,000 | | | |||||||||||||||
| Haitham Elsheikh |
250,000 | * | 250,000 | | | |||||||||||||||
| Michael Rapoport (13) |
250,000 | * | 250,000 | | | |||||||||||||||
| Michael Garnick |
203,576 | * | 203,576 | | | |||||||||||||||
| Sharp Clinical Services (14) |
249,048 | * | 83,016 | 166,032 | * | |||||||||||||||
| Diamond MGT Holdings, LLC (15) |
248,511 | * | 82,837 | 165,674 | * | |||||||||||||||
| ACP Partners Fund, L.P. (16) |
200,000 | * | 200,000 | | | |||||||||||||||
| LGA Investments Family Limited Partnership (17) |
198,100 | * | 198,100 | | | |||||||||||||||
| David M. & Patricia A. Kutz, JTWROS (18) |
200,000 | * | 200,000 | | | |||||||||||||||
| D&R Partners, LLC (19) |
156,667 | * | 156,667 | | | |||||||||||||||
| Dominion Capital, LLC (20) |
166,667 | * | 166,667 | | | |||||||||||||||
| Hillside Ventures Investments SA (21) |
200,000 | * | 200,000 | | | |||||||||||||||
| Rubber Specialists Acquisition LLC (22) |
100,000 | * | 100,000 | | | |||||||||||||||
| Robert deRose & Susan deRose Family Trust 11/18/86 (23) |
148,300 | * | 148,300 | | | |||||||||||||||
| Moonlight Enterprises Ltd. (24) |
200,000 | * | 200,000 | | | |||||||||||||||
| Harbor View Ventures LLC (25) |
166,667 | * | 166,667 | | | |||||||||||||||
| Amnon Mandelbaum (26) |
175,000 | * | 175,000 | | | |||||||||||||||
| Floyd Roos Properties LLC DBP (27) |
174,257 | * | 91,419 | 82,838 | * | |||||||||||||||
| Terry Plasse |
94,623 | * | 24,312 | 71,623 | * | |||||||||||||||
| JKW Family LTD (28) |
140,000 | * | 140,000 | | | |||||||||||||||
| NLBDIT 2010 Enterprises LLC (29) |
131,250 | * | 131,250 | | | |||||||||||||||
| John B. & Judith Goodrich |
124,257 | * | 41,419 | 82,838 | * | |||||||||||||||
| Michael Gregoire |
124,257 | * | 41,419 | 82,838 | * | |||||||||||||||
| Stuart Wolpoff & Lee Rosner JTWROS |
124,254 | * | 41,418 | 82,836 | * | |||||||||||||||
| Equity Trust Company Cust. FBO Lawrence Mintzer IRA |
112,130 | * | 70,710 | 41,420 | * | |||||||||||||||
| Joseph Schump |
100,000 | * | 100,000 | | | |||||||||||||||
| Daniel S. Travelle |
100,000 | * | 100,000 | | | |||||||||||||||
| Vantage Retirement Plans, LLC Cust. FBO Laurence E. Lof, Roth IRA (30) |
100,000 | * | 100,000 | | | |||||||||||||||
| Peter Sabo |
100,000 | * | 100,000 | | | |||||||||||||||
| Troy Taylor |
85,720 | * | 85,720 | | | |||||||||||||||
| Michael Rizzo |
100,000 | * | 100,000 | | | |||||||||||||||
69
Table of Contents
|
Shares Beneficially Owned as of the date of this Prospectus |
Shares Offered by this Prospectus |
Shares Beneficially Owned After the Offering (1) |
||||||||||||||||||
| Name of Selling Stockholder |
Number | Percent | Number | Percent | ||||||||||||||||
| John Burgraff (31) |
100,000 | * | 100,000 | | | |||||||||||||||
| Robert F. Baltera Jr. |
100,000 | * | 100,000 | | | |||||||||||||||
| Jeffry F. Schoenbaum Rev Trust U/A 03/04/96 (32) |
100,000 | * | 100,000 | | | |||||||||||||||
| Dilip & Bhavini Patel |
100,000 | * | 100,000 | | | |||||||||||||||
| Clayton Struve |
100,000 | * | 100,000 | | | |||||||||||||||
| Andrew Fisher & Melissa A. Fisher |
100,000 | * | 100,000 | | | |||||||||||||||
| Cavalry Fund I, LP (33) |
72,567 | * | 72,567 | | | |||||||||||||||
| Sandeep Shah |
98,364 | * | 62,730 | 35,634 | * | |||||||||||||||
| Michael Mark |
74,555 | * | 24,852 | 49,703 | * | |||||||||||||||
| Steven Freifeld (34) |
46,670 | * | 46,670 | | | |||||||||||||||
| Marc R. Cote |
67,278 | * | 42,426 | 24,852 | * | |||||||||||||||
| Bhalchandra G. Parulkar |
64,917 | * | 43,822 | 21,095 | * | |||||||||||||||
| Amar V. Kapur |
64,910 | 43,821 | 21,089 | * | ||||||||||||||||
| Lauer-Williams Family Trust (35) |
64,115 | * | 21,372 | 42,743 | * | |||||||||||||||
| Venture Law, Inc. Defined Pension Plan (36) |
62,130 | * | 20,710 | 41,420 | * | |||||||||||||||
| Richard Fedorowich |
62,127 | * | 20,709 | 41,418 | * | |||||||||||||||
| Karen Donovan |
62,127 | * | 20,709 | 41,418 | * | |||||||||||||||
| Jeff Arnold |
62,127 | * | 20,709 | 41,418 | * | |||||||||||||||
| Donald E. Bates |
62,127 | * | 20,709 | 41,418 | * | |||||||||||||||
| Fort Point Angels LLC (37) |
60,000 | * | 60,000 | | | |||||||||||||||
| Ari Sason |
60,000 | * | 60,000 | | | |||||||||||||||
| LRC 2011 Trust (38) |
57,614 | * | 39,205 | 18,409 | | |||||||||||||||
| Carl M. Berke |
57,246 | * | 19,082 | 38,164 | * | |||||||||||||||
| Philip R. Morgan |
29,411 | * | 20,746 | 8,665 | * | |||||||||||||||
| Peter J. Aranow |
52,400 | * | 20,742 | 31,658 | * | |||||||||||||||
| Vincent Grillo |
50,000 | * | 50,000 | | | |||||||||||||||
| Robert L. Montgomery |
50,000 | * | 50,000 | | | |||||||||||||||
| Chris & Lauren Cates (39) |
50,000 | * | 50,000 | | | |||||||||||||||
| Joseph A. Di Vito, Jr. Personal Trust (40) |
50,000 | * | 50,000 | | | |||||||||||||||
| Fred & Allison Wagner |
50,000 | * | 50,000 | | | |||||||||||||||
| Edwin C. Blitz (41) |
50,000 | * | 50,000 | | | |||||||||||||||
| Stephen M. Andress |
50,000 | * | 50,000 | | | |||||||||||||||
| Tim Elmes, LLC (42) |
50,000 | * | 50,000 | | | |||||||||||||||
| Mitchell Sivertson (43) |
41,700 | * | 41,700 | | | |||||||||||||||
| Jack Springer |
50,000 | * | 50,000 | | | |||||||||||||||
| The Richard M. Spitalny Living Trust dated 11/11/13 (44) |
50,000 | * | 50,000 | | | |||||||||||||||
| Bruce Pedersen |
41,667 | * | 41,667 | | | |||||||||||||||
| Aaron Lehmann |
38,900 | * | 38,900 | | | |||||||||||||||
| Balsam Capital Management (45) |
50,000 | * | 50,000 | | | |||||||||||||||
| Carlos & Tracy Garcia |
33,334 | * | 33,334 | | | |||||||||||||||
| Nicholas Alexander Revocable Trust (46) |
33,334 | * | 33,334 | | | |||||||||||||||
70
Table of Contents
|
Shares Beneficially Owned as of the date of this Prospectus |
Shares Offered by this Prospectus |
Shares Beneficially Owned After the Offering (1) |
||||||||||||||||||
| Name of Selling Stockholder |
Number | Percent | Number | Percent | ||||||||||||||||
| Wollheim Family Trust (47) |
41,667 | * | 41,667 | 8,333 | * | |||||||||||||||
| Andrew H. Kaufman |
50,000 | * | 50,000 | | | |||||||||||||||
| Peter W. Janssen (48) |
50,000 | * | 50,000 | | | |||||||||||||||
| Douglas P. Kaufman |
50,000 | * | 50,000 | | | |||||||||||||||
| John E. & Laura G. Knight (49) |
50,000 | * | 50,000 | | | |||||||||||||||
| Perry Tepper |
50,000 | * | 50,000 | | | |||||||||||||||
| Daniel J. Gilbert |
50,000 | * | 50,000 | | | |||||||||||||||
| Matthew D. MacLean & Regina M. MacLean (50) |
43,900 | * | 43,900 | | | |||||||||||||||
| Northlea Partners (51) |
50,000 | * | 50,000 | | | |||||||||||||||
| Douglas Jay Cohen |
50,000 | * | 50,000 | | | |||||||||||||||
| Itzhak & Galia Shenberg |
50,000 | * | 50,000 | | | |||||||||||||||
| Lantis Consultants Inc. (52) |
50,000 | * | 50,000 | | | |||||||||||||||
| Courtagen Angel Fund 1, LLC (53) |
49,703 | * | 16,568 | 33,135 | * | |||||||||||||||
| McKernan Family Partnership (54) |
49,703 | * | 16,568 | 33,135 | * | |||||||||||||||
| Sunrise Foundation Trust (55) |
43,750 | * | 43,750 | | | |||||||||||||||
| Allen Michel |
41,217 | * | 13,739 | 27,478 | * | |||||||||||||||
| Bruce A. Ferguson, IRA Raymond James & Assoc., Inc. CSDN |
40,000 | * | 40,000 | | | |||||||||||||||
| Clifford L. & Amy J. Caplan (56) |
40,000 | * | 40,000 | | | |||||||||||||||
| Dilip M. Jain & Keshav D. Pandey |
40,000 | * | 40,000 | | | |||||||||||||||
| Ari Zimran Consulting LTD (57) |
40,000 | * | 40,000 | | | |||||||||||||||
| Lisa Kirby-Gibbs |
38,910 | * | 15,154 | 23,756 | * | |||||||||||||||
| Howard Bilow |
37,277 | * | 12,426 | 24,851 | * | |||||||||||||||
| George Xixis |
36,638 | * | 12,213 | 24,425 | * | |||||||||||||||
| Rohit D. Vakil |
34,912 | * | 13,820 | 21,092 | * | |||||||||||||||
| Joel Kovacs |
30,000 | * | 30,000 | | | |||||||||||||||
| John & Gail Deviddio |
30,000 | * | 30,000 | | | |||||||||||||||
| Jayant G. & Bharati J. Phadke |
30,000 | * | 30,000 | | | |||||||||||||||
| Charles S. & Beth A. Hall (58) |
30,000 | * | 30,000 | | | |||||||||||||||
| Prasoon Chaturvedi |
30,000 | * | 30,000 | | | |||||||||||||||
| Neal Tepper |
30,000 | * | 30,000 | | | |||||||||||||||
| Gruh, LLC (59) |
30,000 | * | 30,000 | | | |||||||||||||||
| Michael Zimmerman |
28,500 | * | 28,500 | | | |||||||||||||||
| Andrew & Barbara J. Douglas |
24,852 | * | 8,284 | 16,568 | * | |||||||||||||||
| Berenson Ventures, LP (60) |
24,852 | * | 8,284 | 16,568 | * | |||||||||||||||
| Richard Anders |
24,845 | * | 8,282 | 16,563 | * | |||||||||||||||
| Jeffrey Tarrand |
20,000 | * | 20,000 | | | |||||||||||||||
| Jake Ayre |
20,000 | * | 20,000 | | | |||||||||||||||
| Ian Stern |
20,000 | * | 20,000 | | | |||||||||||||||
| Terence Oi & Patricia Meehan |
16,667 | * | 16,667 | | | |||||||||||||||
| Samuel R. Solis |
20,000 | * | 20,000 | | | |||||||||||||||
| George B. Abercrombie |
20,000 | * | 20,000 | | | |||||||||||||||
71
Table of Contents
|
Shares Beneficially Owned as of the date of this Prospectus |
Shares Offered by this Prospectus |
Shares Beneficially Owned After the Offering |
||||||||||||||||||
| Name of Selling Stockholder |
Number | Percent | Number | Percent | ||||||||||||||||
| Jacob Movtady |
13,334 | * | 13,334 | | | |||||||||||||||
| Alan F. Holmer |
20,000 | * | 20,000 | | | |||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||
| Total |
22,480,643 | 19,470,273 | 3,020,017 | |||||||||||||||||
(1) Share numbers include shares underlying warrants held by the selling stockholder.
(2) Assumes the sale of all shares offered pursuant to this prospectus.
(3) Fred Knoll is a natural person with voting and dispositive power over the shares held by Europa International, Inc.
(4) Laurence G. Allen is a natural person with voting and dispositive power over the shares held by ACP Partners Fund, LP, ACP X, LP, and LGA Investments Family Limited Partnership. Mr. Allen is affiliated with a FINRA member broker-dealer.
(5) James H. Mannix is a natural person with voting and dispositive power over the shares held by Perceptive Life Sciences Master Fund, Ltd.
(6) Theresa OBrien is a trustee with voting and dispositive power over the shares held by the BobCat Property Trust of Angel Fire, New Mexico.
(7) Kimberly Langston is a natural person with voting and dispositive power over the shares held by Rexford Capital, LLC.
(8) Derek J. Sroufe is affiliated with a FINRA member broker-dealer.
(9) Laurence G. Allen is affiliated with a FINRA member broker-dealer.
(10) Jeremy Office is a natural person with voting and dispositive power over the shares held by SJO Worldwide LLC.
(11) Jennifer Lorenzo is a natural person with voting and dispositive power over the shares held by GJG Life Sciences LLC.
(12) Darren Ross is a natural person with voting and dispositive power over the shares held by Titan Perc, Ltd.
(13) Michael Rapoport is affiliated with a FINRA member broker-dealer.
(14) David Thomson is a natural person with voting and dispositive power over the shares held by Sharp Clinical Services.
(15) David Goldstein is a natural person with voting and dispositive power over the shares held by Diamond MGT Holdings, LLC.
(16) Laurence G. Allen is a natural person with voting and dispositive power over the shares held by ACP Partners Fund, LP, ACP X, LP, and LGA Investments Family Limited Partnership. Mr. Allen is affiliated with a FINRA member broker-dealer.
(17) Laurence G. Allen is a natural person with voting and dispositive power over the shares held by ACP Partners Fund, LP, ACP X, LP, and LGA Investments Family Limited Partnership. Mr. Allen is affiliated with a FINRA member broker-dealer.
(18) David Kutz is a FINRA member broker-dealer.
(19) Jeffrey Maller is a natural person with voting and dispositive power over the shares held by D&R Partners, LLC.
(20) Mikhail Gurevich is a natural person with voting and dispositive power over the shares held by Dominion Capital, LLC.
(21) David Ishag is a natural person with voting and dispositive power over the shares held by Hillside Ventures Investments SA.
72
Table of Contents
(22) Raffaele Attar is a natural person with voting and dispositive power over the shares held by Rubber Specialists Acquisition LLC.
(23) Robert deRose is a trustee with voting and dispositive power over the shares held by Robert deRose & Susan deRose Family Trust 11/18/86.
(24) Diego Lissi is a natural person with voting and dispositive power over the shares held by Moonlight Enterprises Ltd.
(25) Donald Schaeffer and Richard Schaeffer are natural persons with voting and dispositive power over the shares held by Harbor View Ventures LLC.
(26) Amnon Mandelbaum is affiliated with a FINRA member broker-dealer.
(27) Warren Roos is a natural person with voting and dispositive power over the shares held by Floyd Roos Properties LLC DBP.
(28) Joshua Weiss is a natural person with voting and dispositive power over the shares held by JKW Family LTD.
(29) Sam Masri is a natural person with voting and dispositive power over the shares held by NLBDIT 2010 Enterprises LLC. Mr. Masri is affiliated with a FINRA member broker-dealer.
(30) Laurence E. Lof is affiliated with a FINRA member broker-dealer.
(31) John Burgraff is affiliated with a FINRA member broker-dealer.
(32) Jeffry Scheonbaum is a trustee with voting and dispositive power over the shares held by the Jeffry F. Schoenbaum Revocable Trust U/A 03/04/96.
(33) Thomas P. Walsh is a natural person with voting and dispositive power over the shares held by Cavalry Fund I, LP.
(34) Steven Freifeld is a FINRA member broker-dealer.
(35) Michael Williams is a trustee with voting and dispositive power over the shares held by the Lauer-Williams Family Trust.
(36) H. Kenneth Merritt and Sharon J. Merritt are co-trustees with voting and dispositive power over the shares held by the Venture Law Inc., Kenneth Merritt Defined Pension Plan.
(37) Oleg Uritsky is a natural person with voting and dispositive power over the shares held by Fort Point Angels LLC.
(38) Lee R. Chartock is a trustee with voting and dispositive power over the shares held by LRC 2011 Trust.
(39) Chris Cates is a FINRA member broker-dealer.
(40) Joseph A. Di Vito, Jr. is a trustee with voting and dispositive power over the shares held by Joseph A. Di Vito, Jr. Personal Trust.
(41) Edwin C. Blitz is a FINRA member.
(42) Tim Elmes is a natural person with voting and dispositive power over the shares held by Tim Elmes, LLC.
(43) Mitchell Sivertson is affiliated with a FINRA member broker-dealer.
(44) Richard M. Spitalny is a trustee with voting and dispositive power over the shares held by The Richard Spitalny Living Trust dated 11/11/13.
(45) Arnold Balsam is a natural person with voting and dispositive power over the shares held by Balsam Capital Management.
(46) Nicholas Alexander is a trustee with voting and dispositive power over the shares held by the Nicholas Alexander Revocable Trust.
(47) Bryan Wollheim is a trustee with voting and dispositive power over the shares held by Wollheim Family Trust. Mr. Wollheim is a FINRA member broker-dealer.
73
Table of Contents
(48) Mr. Janssen is a FINRA member broker-dealer.
(49) Mr. Knight is affiliated with a FINRA member.
(50) Mr. MacLean is a FINRA member.
(51) Dr. John H. Abeles is a natural person with voting and dispositive power over the shares held by Northlea Partners.
(52) Eliezer Tokman is a natural person with voting and dispositive power over the shares held by Lantis Consultants Inc.
(53) Brendan McKernan is a natural person with voting and dispositive power over the shares held by Courtagen Angel Fund 1, LLC and the McKernan Family Partnership.
(54) Brendan McKernan is a natural person with voting and dispositive power over the shares held by Courtagen Angel Fund 1, LLC and the McKernan Family Partnership.
(55) Nathan Low is a natural person with voting and dispositive power over the shares held by Sunrise Foundation Trust. Mr. Low is affiliated with a FINRA member broker-dealer.
(56) Clifford Caplan is affiliated with a FINRA member broker-dealer.
(57) Ari Zimran is a natural person with voting and dispositive power over the shares held by Ari Zimran Consulting LTD.
(58) Charles S. Hall is affiliated with a FINRA member broker-dealer.
(59) Nikita Shah is a natural person with voting and dispositive power over the shares held by Gruh, LLC.
(60) Richard Berenson is a natural person with voting and dispositive power over the shares held by Berenson Ventures, LP.
74
Table of Contents
The selling stockholders, which as used herein includes donees, pledgees, transferees or other successors in-interest selling shares of common stock or interests in shares of common stock received after the date of this prospectus from a selling stockholder as a gift, pledge, partnership distribution or other transfer, may, from time to time, sell, transfer or otherwise dispose of any or all of their shares of common stock or interests in shares of common stock on any stock exchange, market or trading facility on which the shares are traded or in private transactions.
Our common stock is quoted on the OTC.QB under the symbol CRBP. The selling security holders may sell some or all of their shares at prevailing market prices or privately negotiated prices on the OTC.QB.
The selling stockholders may use any one or more of the following methods when disposing of shares or interests therein:
| | ordinary brokerage transactions and transactions in which the broker-dealer solicits purchasers; |
| | block trades in which the broker-dealer will attempt to sell the shares as agent, but may position and resell a portion of the block as principal to facilitate the transaction; |
| | purchases by a broker-dealer as principal and resale by the broker-dealer for its account; |
| | privately negotiated transactions; |
| | short sales; |
| | through the writing or settlement of options or other hedging transactions, whether through an options exchange or otherwise; |
| | broker-dealers may agree with the selling stockholders to sell a specified number of such shares at a stipulated price per share; |
| | a combination of any such methods of sale; and |
| | any other method permitted pursuant to applicable law. |
The selling stockholders may, from time to time, pledge or grant a security interest in some or all of the shares of common stock owned by them and, if they default in the performance of their secured obligations, the pledgees or secured parties may offer and sell the shares of common stock, from time to time, under this prospectus, or under an amendment to this prospectus under Rule 424)(b)(3) or other applicable provision of the Securities Act amending the list of selling stockholders to include the pledgee, transferee or other successors in interest as selling stockholders under this prospectus. The selling stockholders also may transfer the shares of common stock in other circumstances, in which case the transferees, pledgees or other successors in interest will be the selling beneficial owners for purposes of this prospectus; provided, however, that prior to any such transfer the following information (or such other information as may be required by the federal securities laws from time to time) with respect to each such selling beneficial owner must be added to the prospectus by way of a prospectus supplement or post-effective amendment, as appropriate: (1) the name of the selling beneficial owner; (2) any material relationship the selling beneficial owner has had within the past three years with us or any of our predecessors or affiliates; (3) the amount of securities of the class owned by such beneficial owner before the offering; (4) the amount to be offered for the beneficial owners account; and (5) the amount and (if one percent or more) the percentage of the class to be owned by such beneficial owner after the offering is complete.
In connection with the sale of our common stock or interests therein, the selling stockholders may enter into hedging transactions with broker-dealers or other financial institutions, which may in turn engage in short sales of the common stock in the course of hedging the positions they assume. The selling stockholders may also sell shares of our common stock short and deliver these securities to close out their short positions, or loan or pledge the common stock to broker-dealers that in turn may sell these securities. The selling stockholders may also enter into option or other transactions with broker-dealers or other financial institutions or the creation of one or more derivative securities which require the delivery to such broker-dealer or other financial institution of shares offered by this prospectus, which shares such broker-dealer or other financial institution may resell pursuant to this prospectus (as supplemented or amended to reflect such transaction).
The aggregate proceeds to the selling stockholders from the sale of the common stock offered by them will be the purchase price of the common stock less discounts or commissions, if any. Each of the selling stockholders reserves the right to accept and, together with their agents from time to time, to reject, in whole or in part, any proposed purchase of common stock to be made directly or through agents. We will not receive any of the proceeds from this offering, provided, however, we will receive proceeds from the exercise of the warrants held by certain investors.
75
Table of Contents
The selling stockholders also may resell all or a portion of the shares in open market transactions in reliance upon Rule 144 under the Securities Act, provided that they meet the criteria and conform to the requirements of that rule.
The selling stockholders and any underwriters, broker-dealers or agents that participate in the sale of the common stock or interests therein may be underwriters within the meaning of Section 2(11) of the Securities Act. Any discounts, commissions, concessions or profit they earn on any resale of the shares may be underwriting discounts and commissions under the Securities Act. Selling stockholders who are underwriters within the meaning of Section 2(11) of the Securities Act will be subject to the prospectus delivery requirements of the Securities Act.
To the extent required, the shares of our common stock to be sold, the names of the selling stockholders, the respective purchase prices and public offering prices, the names of any agents, dealer or underwriter, any applicable commissions or discounts with respect to a particular offer will be set forth in an accompanying prospectus supplement or, if appropriate, a post-effective amendment to the registration statement that includes this prospectus.
The maximum amount of compensation to be received by any FINRA member or independent broker-dealer for the sale of any securities registered under this prospectus will not be greater than 8.0% of the gross proceeds from the sale of such securities.
In order to comply with the securities laws of some states, if applicable, the common stock may be sold in these jurisdictions only through registered or licensed brokers or dealers. In addition, in some states the common stock may not be sold unless it has been registered or qualified for sale or an exemption from registration or qualification requirements is available and is complied with.
We have advised the selling stockholders that the anti-manipulation rules of Regulation M under the Exchange Act may apply to sales of shares in the market and to the activities of the selling stockholders and their affiliates. In addition, we will make copies of this prospectus (as it may be supplemented or amended from time to time) available to the selling stockholders for the purpose of satisfying the prospectus delivery requirements of the Securities Act. The selling stockholders may indemnify any broker-dealer that participates in transactions involving the sale of the shares against certain liabilities, including liabilities arising under the Securities Act.
76
Table of Contents
MARKET FOR COMMON EQUITY AND RELATED STOCKHOLDER MATTERS
Market Information
Our common stock is quoted on the OTC.QB under the symbol CRBP. Our shares of common stock began being quoted on the OTC.QB under the symbol CRBP effective October 24, 2014.
The following table contains information about the range of high and low bid prices for our common stock for each quarter during the last two years based upon quotations on the OTC.QB.
| Fiscal Quarter Ended | High Sales Price | Low Sales Price | ||
| Fourth Quarter, 2014 |
$4.95 | $2.71 | ||
| First Quarter 2015 (through March 26, 2015) |
$3.25 | $2.00 |
The source of these high and low sales prices was OTC.QB. These quotations reflect inter-dealer prices, without retail mark-up, markdown or commissions and may not represent actual transactions. The high and low sales prices listed have been rounded up to the hundredths. Trades in the common stock may be subject to Rule 15g-9 of the Exchange Act, which imposes requirements on broker/dealers who sell securities subject to the rule to persons other than established customers and accredited investors. For transactions covered by the rule, broker/dealers must make a special suitability determination for purchasers of the securities and receive the purchasers written agreement to the transaction before the sale.
The SEC also has rules that regulate broker/dealer practices in connection with transactions in penny stocks. Penny stocks generally are equity securities with a price of less than $5.00 (other than securities listed on certain national exchanges, provided that the current price and volume information with respect to transactions in that security is provided by the applicable exchange or system). The penny stock rules require a broker/dealer, before effecting a transaction in a penny stock not otherwise exempt from the rules, to deliver a standardized risk disclosure document prepared by the SEC that provides information about penny stocks and the nature and level of risks in the penny stock market. The broker/dealer also must provide the customer with current bid and offer quotations for the penny stock, the compensation of the broker/dealer and its salesperson in the transaction, and monthly account statements showing the market value of each penny stock held in the customers account. The bid and offer quotations, and the broker/dealer and salesperson compensation information, must be given to the customer orally or in writing before effecting the transaction, and must be given to the customer in writing before or with the customers confirmation. These disclosure requirements may have the effect of reducing the level of trading activity in the secondary market for shares of common stock. As a result of these rules, investors may find it difficult to sell their shares.
Dividends
We have never declared or paid cash dividends on our common stock. We do not intend to declare or pay cash dividends on our common stock for the foreseeable future, but currently intend to retain any future earnings to fund the development and growth of our business. The payment of cash dividends if any, on the common stock will rest solely within the discretion of our board of directors and will depend, among other things, upon our earnings, capital requirements, financial condition, and other relevant factors.
Holders
As of March 12, 2015, there were 246 record holders of our common stock.
The validity of the securities offered in this prospectus is being passed upon for us by Lowenstein Sandler LLP, New York, New York.
The consolidated balance sheets of Corbus Pharmaceuticals Holdings, Inc. as of December 31, 2014 and 2013, and the related consolidated statements of operations, preferred stock and stockholders equity (deficit), and cash flows for each of the years in the two-year period ended December 31, 2014, have been audited by EisnerAmper LLP, an independent registered public accounting firm, as stated in their report which is incorporated herein by reference. Such financial statements have been incorporated herein by reference in reliance on the report of such firm given upon their authority as experts in accounting and auditing.
77
Table of Contents
DISCLOSURE OF COMMISSION POSITION ON INDEMNIFICATION FOR SECURITIES ACT LIABILITIES
Our directors and officers are indemnified to the fullest extent permitted under Delaware law. We also maintain insurance which protects our officers and directors against any liabilities incurred in connection with their service in such a capacity.
Insofar as indemnification for liabilities arising under the Securities Act may be permitted to our directors, officers and controlling persons pursuant to the foregoing, or otherwise, we have been advised that in the opinion of the SEC such indemnification is against public policy as expressed in the Securities Act and is, therefore, unenforceable. In the event that a claim for indemnification against such liabilities (other than the payment by us of expenses incurred or paid by a director, officer or controlling person of ours in the successful defense of any action, suit or proceeding) is asserted by such director, officer or controlling person in connection with the securities being registered, we will, unless in the opinion of our counsel the matter has been settled by controlling precedent, submit to a court of appropriate jurisdiction the question whether such indemnification by it is against public policy as expressed in the Securities Act and will be governed by the final adjudication of such issue.
WHERE YOU CAN FIND ADDITIONAL INFORMATION
We have filed with the SEC a registration statement on Form S-1 under the Securities Act, with respect to the common stock offered by this prospectus. This prospectus, which is part of the registration statement, omits certain information, exhibits, schedules and undertakings set forth in the registration statement. For further information pertaining to us and our common stock, reference is made to the registration statement and the exhibits and schedules to the registration statement. Statements contained in this prospectus as to the contents or provisions of any documents referred to in this prospectus are not necessarily complete, and in each instance where a copy of the document has been filed as an exhibit to the registration statement, reference is made to the exhibit for a more complete description of the matters involved.
You may read and copy all or any portion of the registration statement without charge at the office of the SEC at the Public Reference Room at Station Place, 100 F Street, N.E., Washington, D.C. 20549. Copies of the registration statement may be obtained from the SEC at prescribed rates from the Public Reference Section of the SEC at such address. In addition, registration statements and certain other filings made with the SEC electronically are publicly available through the SECs web site at http://www.sec.gov. The registration statement, including all exhibits and amendments to the registration statement, has been filed electronically with the SEC.
We have also filed a Registration Statement on Form 8-A and are now subject to the information and periodic reporting requirements of the Exchange Act and, accordingly, we file annual reports containing financial statements audited by an independent public accounting firm, quarterly reports containing unaudited financial data, current reports, proxy statements and other information with the Securities and Exchange Commission. You can inspect and copy such periodic reports, proxy statements and other information at the SECs public reference room, and the web site of the SEC referred to above.
78
Table of Contents
DOCUMENTS INCORPORATED BY REFERENCE
The SEC allows us to incorporate by reference information into this document. This means that we can disclose important information to you by referring you to another document filed separately with the SEC. The information incorporated by reference is considered to be a part of this document, except for any information superseded by information that is included directly in this document or incorporated by reference subsequent to the date of this document.
This prospectus incorporates by reference the documents listed below:
| | our Annual Report on Form 10-K for the year ended December 31, 2014, filed with the SEC on February 10, 2015; and |
| | our Current Reports on Form 8-K filed with the SEC on January 5, 2015, February 9, 2015 and February 10, 2015 (other than any portions thereof deemed furnished and not filed). |
You should rely only on the information incorporated by reference or provided in this prospectus. We have not authorized anyone to provide you with different information. You should not assume that the information in this prospectus is accurate as of any date other than the date on the front of this document. Any statement contained in a document incorporated in this prospectus will be deemed to be modified or superseded for purposes of this prospectus to the extent that a statement contained in this prospectus modifies or supersedes that statement. Any statement that is modified or superseded will not constitute a part of this prospectus, except as modified or superseded.
You may request a copy of these filings, at no cost, by writing or calling us at the following:
Corbus Pharmaceuticals Holdings, Inc.
100 River Ridge Drive
Norwood, Massachusetts 02062
Attn: Sean Moran
E-mail: smoran@corbuspharma.com
Phone: (617) 963-0100
Copies of the documents incorporated by reference may also be found on our website at www.corbuspharma.com. Except with respect to the documents expressly incorporated by reference above which are accessible at our website, the information contained on our website is not a part of, and should not be construed as being incorporated by reference into, this prospectus.
You may read and copy any materials we file with the SEC without charge at the office of the SEC at the Public Reference Room at Station Place, 100 F Street, N.E., Washington, D.C. 20549. You can also obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330. In addition, our filings made with the SEC electronically are publicly available through the SECs web site at http://www.sec.gov.
79
Table of Contents
CORBUS PHARMACEUTICALS HOLDINGS, INC.
19,470,273 Shares
Common Stock
PROSPECTUS
April 6, 2015